


Mustafa T. Sahin1, Serap Ozturkcan1, Ahmet Seyhan2, Peyker Demireli3 and Aylin Turel-Ermertcan1
Departments of 1Dermatology, 2Plastic Surgery and 3Pathology, Medical Faculty, Celal Bayar University, Manisa, Turkey. E-mail: mustafaturhan@superonline.com
Accepted October 24, 2005.
Sir,
Subungual melanoma is a relatively rare disease with a reported incidence of between 0.7% to 3.5% of all melanoma cases in the general population (1). Most common sites of involvement are the big toe, the thumb and the index and ring fingers, respectively (2–4). Common signs include pigmentation of the nail bed, nail loss, and nail destruction, which is sometimes misdiagnosed as onychomycosis (5–7). Subungual melanoma has been associated with a poor prognosis, with a 10–30% 5-year survival, usually attributed to the delay in diagnosis (8–11). Early dermoscopic examination and biopsy of suspicious lesions, followed by amputation of the digit in those proving positive is the treatment of choice (8).
CASE REPORT
A 65-year-old woman presented with a longitudinal melanotic lesion of the nail bed of the left index finger for one year, associated with destruction of the overlying nail. Dermoscopic examination revealed longitudinal pigmented streaks in the entire nail plate with haphazard pigmentation distributed in a disorderly fashion on the cuticle and proximal nail fold (Hutchinson’s sign). She was diagnosed as having subungual melanoma in situ. As the patient had already had an ipsilateral mastectomy one week earlier with removal of axillary lymph nodes because of breast carcinoma, she rejected the nail plate biopsy. Approximately 2 years later when she attended the plastic surgery outpatient clinic, there was a tumour, 5 cm in size, involving the entire distal phalanx and distal half of the middle phalanx (Fig. 1). Histopathological examination, revealed hyperkeratosis, the surface epithelium was irregularly acanthotic, with proliferation of atypical melanocytic cells at the dermoepidermal junction, and there were foci of junctional nest formation. In the dermis, there was extensive proliferation of atypical melanocytic cells some of which were invading the epidermis. There was extension of tumour cells into the reticular dermis (Clark level IV). Its greatest thickness was 4 mm. Mitotic figures averaged 5 per high-power field. Moreover, there was histological ulceration correlating with the thickness of the tumour. Immunohistochemical studies revealed strong HMB-45 positivity of the tumour cells (Fig. 2). According to these histopathological findings she was diagnosed as having subungual melanoma. Afterwards, she underwent finger amputation proximal to the metacarpophalangeal joint (Fig. 3) and antecubital lymphadectomy. Histopathologic examination of her left antecubital lymphadectomy specimen revealed tumour cells consistent with malignant melanoma. Immunohistochemical study was positive for HMB-45.
Fig. 1. The tumour, involving the entire distal phalanx and distal half of the middle phalanx.

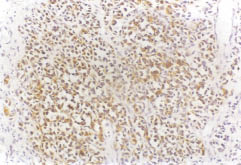
Fig. 2. Strong HMB-45 positivity of the tumour cells (×200).

Fig. 3. Macroscopy of the amputation material shows tumoral invasion, involving the deep tissues of the distal phalanx, interphalangeal articulation and distal portion of the middle phalanx.
DISCUSSION
An important clue to the diagnosis of subungual melanoma is Hutchinson’s sign, which is characterized by extension of brown-black pigment from the nail bed, matrix and nail plate onto the adjacent cuticle and proximal and/or lateral nail folds (12). In our patient, Hutchinson’s sign was very apparent.
Prominent dermoscopic features observed in melanoma are the association of brown pigmentation of the background with longitudinal brown to black lines irregular in their coloration, spacing, thickness and parallelism. A rare feature, micro-Hutchinson sign as defined by the visibility of a pigmentation of the cuticle only on dermoscopy, can also be observed in subungual melanoma (13). Dermoscopic examination of our patient’s longitudinal pigmented lesion revealed irregularly thick, spaced, parallel and coloured lines associated with a brown background.
The prognosis of subungual melanoma is poor because most lesions are at an advanced stage at the time of diagnosis (14). Approximately 75% of primary tumours have been found to be more than 1.5 mm thick, 61% invading to level IV or V (13). As with all types of melanoma, there is strong relationship between increasing tumour thickness and decreasing survival time. Six prognostic factors, including tumour thickness, stage at presentation, presence of ulceration, bone invasion, and high aneuploid fraction and a low S-phase fraction in DNA studies, had been found to be greatly affecting patient survival. Although subungual melanoma in our patient was diagnosed early, she was operated at an advanced stage as a result of her delay in presentation, contributing to the poor prognosis.
We believe that early dermoscopic examination and biopsy of suspicious lesions, followed by amputation of the digit in those proving positive, lead to the only possibility of curative treatment of subungual melanoma.
REFERENCES
1. Levit EK, Kagen MH, Scher RK, Grossman M, Altman E. The ABC rule for clinical detection of subungual melanoma. J Am Acad Dermatol 2000; 42: 269–274.
2. Blessing K, Kernohan NM, Park KG. Subungual malignant melanoma: clinicopathological features of 100 cases. Histopathology 1991; 19: 425–429.
3. Finley RK 3rd, Driscoll DL, Blumenson LE, Karakousis CP. Subungual melanoma: an eighteen-year review. Surgery 1994; 116: 96–100.
4. Krige JE, Hudson DA, Johnson CA, King HS, Chetty R. Subungual melanoma. S Afr J Surg 1995; 33: 10–14.
5. Grant-Kels JM, Bason ET, Grin CM. The misdiagnosis of malignant melanoma. J Am Acad Dermatol 1999; 40: 539–548.
6. Linares MD, Hardisson D, Perna C. Subungual malignant melanoma of the hand: unusual clinical presentation. Case report. Scand J Plast Reconstr Surg Hand Surg 1998; 32: 347–350.
7. Horton S, Mizuguchi R, Moiin A, Hashimoto K. Erythematous nodule on the nail bed. Arch Dermatol 1999; 135: 1113–1118.
8. Campbell WJ, Harper CV, Alderdice JM, Humphreys WG. Subungal melanoma. Ir J Med Sci 1990; 159: 145–146.
9. Rigby HS, Briggs JC. Subungual melanoma: a clinico-pathological study of 24 cases. Br J Plast Surg 1992; 45: 275–278.
10. Paul E, Kleiner H, Bodeker RH. Epidemiologie und Prognose subungualer Melanome. Hautarzt 1992; 43: 286–290.
11. Metzger S, Ellwanger U, Stroebel W, Schiebel U, Rassner G, Fierlbeck G. Extent and consequences of physician delay in the diagnosis of acral melanoma. Melanoma Res 1998; 8: 181–186.
12. Boran T, Kechijian P. Hutchinson’s sign: a reappraisal. J Am Acad Dermatol 1996; 34: 87–90.
13. Ronger S, Touzet S, Ligeron C, Balme B, Viallard AM, Barrut D, et al. Dermoscopic examination of nail pigmentation. Arch Dermatol 2002; 138: 1327–1333.
14. Ishihara Y, Matsumoto K, Kawachi S, Saida T. Detection of early lesions of “ungual” malignant melanoma. Int J Dermatol 1993; 32: 44–47.
*Presented as a poster at the 60th Annual Meeting of the American Academy of Dermatology, New Orleans, LA, USA, February 22–27, 2002.

