


Olga A. Kerr, Megan Mowbray and Michael J. Tidman
Department of Dermatology, Royal Infirmary, Lauriston Building, 1 Lauriston Place, EH3 9HA, Edinburgh, UK. E-mail: olga.kerr@doctors.org.uk
Accepted November 11, 2005.
Sir,
Endometriosis is common, and extrapelvic deposits may occur in up to 12% of affected women. Cutaneous endometriosis is rare, usually appearing in surgical scars or following procedures such as hysterectomy, caesarean sections, episiotomy and laparoscopy. It is probably the result of implantation of viable endometrial cells or their transport via vascular channels. Umbilical endometriosis is rare, with an estimated incidence of 0.5–1% of all patients with endometrial ectopia (1). It can occur after surgery but is generally spontaneous. There is an important differential diagnosis, which includes malignant melanoma, and a metastatic deposit from a systemic malignancy, in particular a gastrointestinal primary tumour, should be considered. We report here a case of umbilical endometriosis in a young woman whose past medical history was unremarkable and highlight how important an accurate history can be in determining correct diagnosis.
CASE REPORT
A 28-year-old woman presented with a 3-year history of a pigmented umbilical nodule. This was associated with cyclical changes in size and occasional pain. There was no associated bleeding. Past medical history and surgical history were unremarkable. On examination there was a 6 mm × 8 mm, soft, dome-shaped light-brown nodule in the umbilicus with no specific dermatoscopic features (Fig. 1).
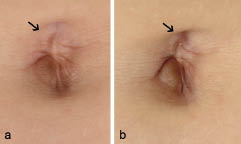
Fig. 1. Umbilical nodule (arrows) at inter-menstrual stage (a) and during menstruation (b).
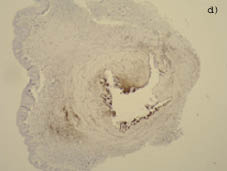
Haematoxylin-eosin staining of the biopsy specimen revealed glandular structures within lower dermis and subcutis with surrounding stromal change, low power and high power magnification showing shedding of the endometrium (Fig. 2). Differentiation of endometrium is readily made by the immunohistochemical demonstration of positive cytokeratin 7, CA125 and CD10 staining and negative cytokeratin 20 staining (Fig. 3).
Fig. 2. Haematoxylin and eosin high-power magnification (×40) showing glandular structures within lower dermis and subcutis with surrounding stromal change and shedding of the endometrium.
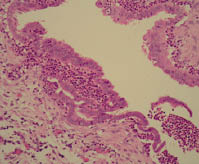
Fig. 3. CD10 is a marker of endometrial stromal cells.
DISCUSSION
Umbilical endometriosis is often slightly tender and painful, and at the time of menstruation the pain becomes more pronounced and may be associated with swelling and slight bleeding occasionally raising the possibility of malignant melanoma (2). The rare possibility of a metastatic deposit from a gastrointestinal primary tumour should also be considered. A recent study has suggested a distinctive dermatoscopic feature in cutaneous endometriosis, comprising small red globular structures, which have been called “red atolls” (3). A detailed examination of material from 10 cases of cutaneous endometriosis revealed a range of histopathological features similar to those found within the uterine endometrium at each of the main phases of the menstrual cycle may be seen (4). Simple excision of umbilical endometriosis, with sparing of the umbilicus when possible, is the treatment of choice. Local recurrence after adequate surgery is uncommon. The coexistence of gynaecological symptoms, such as menorrhagia, dysmenorrhoea or dyspareunia, should prompt investigation to exclude the possibility of pelvic endometriosis.
Cutaneous endometriosis should thus be included in the differential diagnosis of an abdominal lesion that exhibits cyclical variation. The presence of cutaneous endometriosis is not necessarily associated with endometriosis elsewhere. Most cases of cutaneous endometriosis appear in surgical abdominal scars or the umbilicus. Cutaneous endometriosis usually has a distinctive pattern on epiluminescence with small red globular structures lying within homogeneous reddish pigmentation.
References
1. Michowitz M, Baratz M, Stavorovsky M. Endometriosis of the umbilicus. Dermatologica 1983; 167: 326–330.
2. Friedman PM, Rico MJ. Cutaneous endometriosis. Dermatol Online J 2000; 6: 8.
3. De Giorgi V, Massi D, Mannone F, Stante M, Carli P. Cutaneous endometriosis: non-invasive analysis by epiluminescence microscopy. Clin Exp Dermatol 2003; 28: 315–317.
4. Tidman MJ, MacDonald DM. Cutaneous endometriosis: a histopathologic study. J Am Acad Dermatol 1988; 18: 373–377.

