


Per Helsing1 and Erik W. Nielsen2
1Department of Dermatology, Rikshospitalet University Hospital, NO-0027 Oslo, and 2Department of Anaesthesiology, Nordlandssykehuset HF, NO-8092 Bodø and University of Tromsø, Norway. E-mail: per.helsing@rikshospitalet.no
Accepted January 16, 2006.
Sir,
Hereditary angio-oedema (HAE) is a potentially life-threatening disease manifesting as recurrent attacks of laryngeal, intra-abdominal, facial or peripheral oedema. The disease is caused by mutations in the gene coding for C1-inhibitor, resulting in low antigenic or functional concentrations of this inhibitor of complement and kinin systems. Long-term prophylactic treatment is indicated in patients with frequent or severe attacks. Attenuated androgens, anti-fibrinolytic agents and C1-inhibitor concentrates may be used prophylactically. Attenuated androgens are usually effective, but are associated with adverse effects, such as weight gain, virilization in women, arterial hypertension and hepatotoxicity. Danazol is considered a significant risk factor for atherosclerosis, caused by unfavourable changes in the serum lipid profile (1). More recently, hepatocellular adenomas and carcinomas have been reported in patients with HAE, taking danazol for long-term prophylaxis (2, 3).
Focal nodular hyperplasia (FNH) is a common benign tumour of the liver, with unknown pathogenesis (4). There are a few reports linking FNH to use of anabolic androgens (5, 6) and high endogenous sex steroids (7), even to prolonged therapy with ketoconazole (8).
We report here a patient with HAE on long-term prophylaxis with danazol, who developed FNH.
Case report
A 32-year-old woman was diagnosed with HAE at the age of 16 years. Since then she has been taking danazol (Danol®, Sanofi-Synthelabo, New York) on a regular basis at a dosage of 400 mg daily. At lower dosages, she experienced abdominal cramps and swellings in the skin. She gained weight and stopped menstruating after introduction of danazol. At the age of 30 years she was diagnosed with polycystic ovarian syndrome, and clinical examination showed an atrophic uterus. She showed signs of virilization, with acne and hirsutism. Her serum lipid profile was abnormal with high total and low-density lipoprotein (LDL) cholesterol, and she was under treatment for arterial hypertension.
The patients´ liver was monitored by transaminases and an annual ultrasonography. Transaminases were normal, but a tumour was found in the right liver lobe located centrally. Magnetic resonance tomography (Fig. 1) could not differentiate between a hepatocellular adenoma and FNH, but an ultrasonography guided biopsy showed FNH. Danazol was then reduced to 100 mg daily, and the patient was instructed to administer infusions of C1-inhibitor concentrate (Berinert®, ZLB-Behring. Marburg, Germany) intravenously. Disease control was obtained by 1000 IE Berinert® every fourth day. Ultrasonographic follow-up showed no progression of the tumour after 1 year.
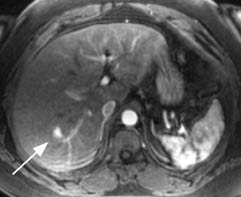
Fig. 1. Focal nodular hyperplasia (arrow) demonstrated by dynamic contrast-enhanced magnetic resonance imaging. (Courtesy of H. J. Smith, MD, Department of Radiology, Rikshospitalet University Hospital, Oslo.
Discussion
Recent reports have documented the association between danazol and the development of hepatocellular adenomas and carcinomas in patients with HAE (2, 3). The risk seems to increase if taking danazol for more than 10 years, at dosages of more than 100 mg.
FNH is a rather common benign tumour of the liver with unknown pathogenesis, encountered in as much as 3% of the general population (4). FNH has been associated with long-term therapy with sex steroids (androgens and oestrogens) and ketoconazole. The associations are mainly case reports and the associations may be coincidental.
Our patient had been taking danazol for more than 10 years in rather high dosage. The accepted association between attenuated androgens and hepatocellular adenomas and carcinomas, leads us to believe there is a causal relationship between long-term prophylaxis with danazol and the development of FNH in this patient. This underlines the importance of regular liver surveillance in patients with HAE on long-term prophylaxis with androgens.
References
1. Szeplaki G, Varga L, Valentin S, Kleiber M, Karadi I, Romics L, et al. Adverse effects of danazol prophylaxis on the lipid profiles of patients with hereditary angio-oedema. J Allergy Clin Immunol 2005; 115: 864–869.
2. Bork K, Pitton M, Harten P, Koch P. Hepatocellular adenomas in patients taking danazol for hereditary angio-oedema. Lancet 1999; 353: 1066–1067.
3. Bork K, Schneiders V. Danazol-induced hepatocellular adenoma in patients with hereditary angio-oedema. J Hepatol 2002; 36: 707–709.
4. Choi BY, Nguyen MH. The diagnosis and management of benign hepatic tumors. J Clin Gastroenterol 2005; 39: 401–412.
5. Alberti-Flor JJ, Iskandarani M, Jeffers L, Zeppa R, Schiff ER. Focal nodular hyperplasia associated with the use of a synthetic anabolic androgen. Am J Gastroenterol 1984; 79: 150–151.
6. Bartley J, Loddenkemper C, Lange J, Mechsner S, Radke C, Neuhaus P, et al. Hepatocellular adenoma and focal nodular hyperplasia after long-term use of danazol for endometriosis: a case report. Arch Gynecol Obstet 2004; 269: 290–293.
7. Grange JD, Guechot J, Legendre C, Giboudeau J, Darnis F, Poupon R. Liver adenoma and focal nodular hyperplasia in a man with high endogenous sex steroids. Gastroenterology 1987; 93: 1409–1413.
8. Machado MC, Jukemura J, Bacchella T, Leite KR, Machado MA, Hayek OR, et al. Focal nodular hyperplasia of the liver observed in a patient undergoing prolonged therapy with ketoconazole. Rev Hosp Clin Fac Med Sao Paulo 1990; 45:132–134.

