


Marianne Kragh Thomsen1, Mads Rasmussen2, Kurt Fuursted1, Henrik Westh3, Lisbeth Nørum Pedersen1, Mette Deleuran2 and Jens Kjølseth Møller1
Departments of 1Clinical Microbiology and 2Dermatology, Aarhus University Hospital, and 3Department of Clinical Microbiology, Hvidovre Hospital, Denmark
In November 2000, we became aware of isolates of Staphylococcus aureus with borderline resistance to oxacillin (BORSA) from patients in the Department of Dermatology, Aarhus University Hospital. The objective was to describe the isolates phenotypically and genotypically and to assess possible transmission routes in order to intervene and prevent further spread. Clonality of the isolates was confirmed by pulsed field gel electrophoresis. Several breaches in infection control procedures were revealed suggesting both direct and indirect transmission between patients. Defective skin barriers, high carrier rates of S. aureus in dermatological patients and high consumption rates of dicloxacillin in the department might facilitate transmission. Following improvement of the general infection control measures, and after reassessment of the antibiotic policy in the department, the outbreak has disappeared. Key words: infection control; antibiotic policy; pulsed field gel electrophoresis.
(Accepted December 20, 2005.)
Acta Derm Venereol 2006; 86: 230–234.
Marianne Kragh Thomsen, Department of Clinical Microbiology, Aarhus University Hospital, Brendstrupgaardsvej 100, DK-8200 Aarhus N, Denmark. E-mail: mkt@dadlnet.dk
Misuse of antibiotics and inadequate hygienic measures in hospitals lead to increased occurrence and spread of drug-resistant micro-organisms (1, 2). An important part of the work of the clinical microbiologist is infection control management (3, 4). One of the surveillance tools is automatically generated reports based on microbiological test results registered in the microbiological laboratory information system (LIS). However, the most sensitive method for detection of outbreaks, either with unusual micro-organisms or micro-organisms with unusual resistance patterns is often alertness in laboratory work and in the contact with the clinicians (3).
In November 2000, we became aware of S. aureus isolates with reduced susceptibility to oxacillin in the Department of Dermatology, Aarhus University Hospital. The phenotypical characteristic that drew attention to the isolates was no zone to a 1 µg oxacillin disc. The lack of the mecA gene indicated that the strains were not methicillin-/multiresistant S. aureus (MRSA).
In this paper we describe the clonal spread of a borderline oxacillin resistant S. aureus (BORSA) strain among patients in the dermatological hospital unit and evaluate the infection control interventions introduced to prevent further spread.
MATERIALS AND METHODS
Patient characteristics
Data on all S. aureus isolates from the Department of Dermatology were extracted from the clinical microbiology unit’s LIS (5). For the 15 patients with isolates of S. aureus with reduced susceptibility to oxacillin detected from November 2000 to October 2001, medical records at the Department of Dermatology and requisition forms received in the Department of Clinical Microbiology were reviewed retrospectively. For each patient the following information was retrieved: date of birth, sex, dates of admission and discharge, dates of visits to the out-patient clinic, date of first positive isolate, sample origin, dermatological diagnosis, immunosuppressive therapy and treatment with antibiotics.
Setting
In 2001, the Department of Dermatology, Aarhus University Hospital had a capacity of 32 beds, corresponding to 1800 admissions per year. Furthermore, the department had a large out-patient clinic with 30,000 contacts per year. Mean overall occupancy rate of the in-patient unit was 85% and the average length of stay was 5.5 days. Statistics of antibiotic consumption of the department were available from the Danish Medicines Agency.
Intervention
The infection control nurse visited the Department of Dermatology and searched for breaches in infection control procedures and possible routes of transmission. Subsequently, two meetings were arranged in 2001 and 2002 with the participation of the infection control nurse and doctors and nurses from the Department of Dermatology, as well as from the Department of Clinical Microbiology, where intervention strategies were discussed and planned.
Laboratory methods
Susceptibility to oxacillin was examined with the disc diffusion method (1 µg disc, Oxoid) on IsoSensitest agar without blood (Oxoid) and confirmed on Columbia agar according to the laboratory standard operating procedures (The Swedish Reference Group for Antibiotics (SRGA) and its subcommittee on methodology (SRGA-M) www.srga.org, updated April 20, 2005). The agar plates were examined in good light to detect thin films of growth or microcolonies within the inhibition zone. Interpretation was performed in duplicate by a skilled laboratory technician and by one of the authors (MKT). Disc diffusion was also used for the antibiogram with Oxoid discs on IsoSensitest agar with blood (Oxoid). Presence of the mecA gene was examined by an in-house PCR assay with amplification of the mecA gene and subsequent amplicon detection by agarose gel electrophoresis.
All the isolates were bacteriophage typed at the Staphylococcal Laboratory, Statens Serum Institut, Copenhagen, Denmark, according to the method of Blair & Williams (6). Pulsed field gel electrophoresis (PFGE) was performed as previously described (7, 8). The spa typing was also performed as previously described (9), except that PCR products were enzymatically purified (Amersham Biosciences, UK) prior to sequencing. Sequence reactions were performed on both DNA strands and analysed on an ABI Prism 3100 (Applied CE Biosystems). For PCR and sequencing of the spa gene, primers 1113F and 1496R (GenBank accession no. J01786) were used. Designation of spa type was carried out using the Ridom Staph Type program (Ridom GmbH, Würzburg, Germany) (10). Sequences representing new spa type sequences were submitted to the Ridom database (www.ridom.de/spaserver, updated June 23, 2005) and after validation assigned new spa type numbers.
RESULTS
Patient characteristics and laboratory results
The first registered S. aureus isolate with reduced susceptibility to oxacillin was from a chronic leg ulcer in a 79-year-old woman in November 2000. She was not treated with antibiotics before the isolate was obtained. The patient had been referred from another county.
Table I shows demographic data of the first 15 patients, comprising 7 men and 8 women with a mean age of 72 years (range 24–89 years). Most of the patients had severe, chronic dermatological illnesses. Ten of the patients received systemic immuno-suppressive medications and four others used topical immuno-suppressive agents (chlormethine and group III steroids). Ten of the patients received low-dose penicillinase-stable penicillins for weeks to months. The samples originated from wounds/skin, blood and urine.
Table I also shows data for phage typing of the S. aureus isolates. Twelve of the isolates were of phage type 95; one was 95/93, and two were non-typeable. We found two different spa types; including a novel one that was submitted to the Ridom SpaServer database (www.ridom.de/spaserver, updated June 23, 2005) as t424 (spa-repeats 08-16-02-16-34-34-17-16-34). The dominant spa type was t230 (spa-repeats 08-16-02-16-34) accounting for 14 of 15 isolates. All the isolates were penicillin resistant and had reduced susceptibility to oxacillin and fusidic acid, but were susceptible to cefoxitin, erythromycin, tetracyclin, clindamycin, streptomycin, gentamicin, rifampicin, vancomycin and linezolid. None of the isolates carried the gene for oxacillin resistance (mecA gene).
Table I. Demographics of the patients, including origin of the samples and data for the phage type of the 15 S. aureus with reduced susceptibility to oxacillin and fusidic acid and resistant to penicillin
Age/Sex Sample origin Dermatological diagnosis Phage-type
79/F Wound Chronic leg ulcer 95
43/M Blood Dermatitis atopica 95
86/F Wound Mycosis fungoides 95
75/F Wound Eczema nummulatum 95/93
58/F Skin Eczema nummulatum 95
24/M Skin Dermatitis atopica 95
89/M Urine SSSS and secondary 95
herpes simplex
81/M Skin Pemphigoides bullosa 95
54/F Wound Dermatomyositis 95
75/M Blood Mycosis fungoides 95
30/F Blood Mb. Darier 95
59/M Wound Lupus erytromatosus 95
disseminatus
72/F Blood Pemphigoides bullosa NTa
75/F Skin Erythrodermia presezary NT
43/M Skin Dermatitis atopica 95
SSSS: Staphylococcal scalded skin syndrome; NT: non-typeable.
aAnother spa-type rather than t230 (t424).
Pulsed field gel electrophoresis patterns were very similar (Fig. 1).
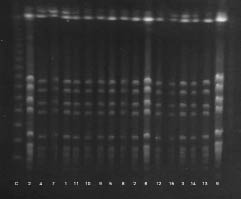
Fig. 1. Pulsed field gel electrophoresis patterns of the 15 isolates of S. aureus with reduced susceptibility to oxacillin after treatment with the restriction enzyme SmaI. Number 2 and 9 were in doublet as controls. The identification numbers of the strains are shown below the gel. The band to the left is the lambda ladder control (C). The patterns show overall similarity with respect to number and position of bands.
Fig. 2 shows mutual coincidence between the patients’ contacts to the dermatological hospital unit prior to the first positive sample. Patient 5 had no admissions, but visited the outpatient clinic on the same day as patient 7 (October 16, 2001).
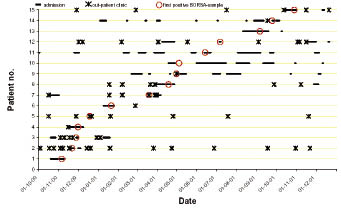
Fig. 2. Time-relationships between the patients contact with the Department of Dermatology (in-patient unit and out-patient clinic) and first positive sample shown for the 15 patients with S. aureus with reduced susceptibility to oxacillin. The figure shows mutual coincidence between the patients’ contacts prior to the first positive sample.
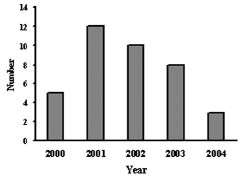
Fig. 3 shows the number of first-time isolates of S. aureus with reduced susceptibility to oxacillin from 2000 to 2004. For five patients we retrieved such isolates after intervals of more than 3 months. There has been a decreasing tendency over time despite no change in sample frequency. For the second half of 2004 we have not detected any isolates with reduced susceptibility to oxacillin.
Fig. 3. Number of first-time S. aureus isolates with reduced susceptibility to oxacillin in the Department of Dermatology. Infection control interventions were launched in autumn 2001 and summer 2002.
Antibiotic consumption
Dicloxacillin consumption per year, in the Department of Dermatology, varied between 1100 and 1670 Defined Daily Doses (DDD) without a specific trend in the period 1996–2004. Use of other betalactams was 570–1090 DDD/year and the use of non-betalactam antibiotics was 430–1800 DDD/year (data not shown).
Infection control procedures
The examination of the dermatological unit by the infection control nurse revealed a large number of potential transmission routes and reservoirs. Firstly, the patients admitted to the dermatological unit often remained together in the unit’s living rooms rather than in their own rooms. The patients were often observed to share creams and lotions and to help each other to apply topical medicines and lotions, in spite of the hospital’s infection control procedures. Worn upholstery furniture was common. The unit was housed in old buildings. There were no single rooms and none of the rooms had direct access to a bathroom. Most of the infected patients were treated with baths containing potassium permanganate. Thorough cleaning of the bath between patients was enforced and patients known to be culture positive with resistant bacteria were treated at the end of the daily programme.
DISCUSSION
A clonal spread of a S. aureus with reduced susceptibility to oxacillin was analysed by PFGE, phage and spa typing among patients in a dermatological hospital unit. The S. aureus strains belonging to the clone were immediately identified through similar patterns of drug resistance toward penicillin, oxacillin and fusidic acid, and an overall similarity in number and position of bands in the pulsed field gel electrophoresis. The spa type t424 was very similar to the predominant spa type t230, but had four repeats in excess. Phage type 95 predominated, but the number of non-typeable strains illustrates the limitations and the less discriminative power of phage typing, which is well-recognized (11). Spa typing seems to constitute a supplement to PFGE for investigation of future outbreaks and local epidemiology of S. aureus.
Many possible routes of transmission were revealed, but we were unable to clarify whether the clonal spread was from patient to patient, through healthcare workers or by shared objects (e.g. creams and lotions). As one of the patients only visited the out-patient clinic, we believe that transmission took place both in the dermatological bed unit, as well as in the out-patient clinic.
To prevent further spread, several interventions were launched. It was recommended that in-patients should be discharged as soon as possible. The antibiotic policy was tightened up, focusing on cessation of antibiotic treatment, if possible, and if necessary, shorter treatment periods of 5 days were recommended. Furthermore, staff and patients were instructed in strict hand hygiene and disinfection of shared objects. Creams and lotions were reserved for personal use only and all upholstered furniture was removed. Again in early autumn 2004 a campaign focusing on hand hygiene was executed at the hospital to raise the general level of infection control. Other authors have concluded that control of nosocomial infection with S. aureus requires a combination of measures, none of which are effective as stand-alone procedures (1).
Spread of the clone in the dermatological unit could have been facilitated by long-time treatment with betalactam antibiotic in low doses, defective skin barriers, close relationships between patients during admission and immuno-suppressive treatment. There was a considerable consumption of dicloxacillin in the dermatological unit, accounting for about half of the total use of antibiotics. Many of our patients were treated with antibiotics more or less continuously over months or years. The antibiotics were, in part, prescribed by their general practitioners and were not taken into account in the above-mentioned consumption statistics. In general the oral dicloxacillin dose was low, 500 mg thrice daily. Long intervals with concentrations below the minimum inhibitory concentration will select resistant mutants. Recently, Guillemot et al. (2) have shown that use of the amoxicillin-clavulanate combination can select for S. aureus strains producing high levels of penicillinase.
Patients with defective skin barriers are prone to be colonized or infected with S. aureus. Patients with severe atopic dermatitis have S. aureus colonization rates as high as 80–100% and most of these patients harbour the bacteria on skin and in the anterior nares (12). Due to the higher carrier rates and scaly skin, they also spread more staphylococci to their surroundings. The contacts of patients with atopic dermatitis have been shown to carry the same strains as the patients (12, 13). These circumstances and the fact that many of the patients are treated with immunosuppressive agents make the dermatological unit prone to staphylococcal outbreaks and necessitate compliance with infection control rules.
We did not investigate the staff for carrier status and we performed no cultures from the environment. This could have revealed other reservoirs and routes of transmission. As we did not systematically screen all the patients in the department, there might have been other patients who harboured the clone. Retrospectively, it was not possible to detect whether the patients carrying the clone shared rooms, since room numbers were not recorded.
Recently, Balslev et al. (14) have reported an outbreak with borderline oxacillin resistant S. aureus in another Danish dermatological unit. Based on the same typing methods, this was shown to be another clone. Balslev et al. concluded that patients with S. aureus with reduced susceptibility to oxacillin had a more severe skin disease, were admitted to hospital more often and had longer duration of hospital stay than a control group of patients with oxacillin susceptible S. aureus.
The patients in our dermatological unit, infected with S. aureus isolates with reduced susceptibility to oxacillin, were treated with dicloxacillin. We experienced no treatment failures, which agrees with findings by other authors (15–17). However, S. aureus with reduced susceptibility to oxacillin is still poorly defined in many respects and the clinical significance and treatment of infections is not clarified.
In conclusion, we evaluated the spread of a clone of borderline oxacillin resistant S. aureus among patients in a dermatological hospital unit. Many possible routes of transmission were revealed. Some of the obvious routes were direct patient-to-patient contact when patients helped each other to apply creams and lotions and indirectly through shared topical medications and worn upholstery furniture. The many facilitating factors in the dermatological department render it prone to outbreaks with S. aureus. Through strengthened focus on general infection control measures and tightened antibiotic policy, the outbreak has disappeared.
ACKNOWLEDGEMENT
We thank Marianne Bøgild, laboratory technician, for assistance with interpretation of the agar plates.
REFERENCES
1. Rampling A, Wiseman S, Davis L, Hyett AP, Walbridge AN, Payne GC, et al. Evidence that hospital hygiene is important in the control of methicillin-resistant Staphylococcus aureus. J Hosp Infect 2001; 49: 109–116.
2. Guillemot D, Bonacorsi S, Blanchard JS, Weber P, Simon S, Guesnon B, et al. Amoxicillin-clavulanate therapy increases childhood nasal colonization by methicillin-susceptible Staphylococcus aureus strains producing high levels of penicillinase. Antimicrob Agents Chemother 2004; 48: 4618–4623.
3. Kolmos HJ. Interaction between the microbiology laboratory and clinician: what the microbiologist can provide. J Hosp Infect 1999; 43 (suppl): S285–291.
4. Mehtar S. Minimum standards in laboratories for infection control. J Hosp Infect 1999; 43 (suppl): S279–283.
5. Moller JK. A microcomputer-assisted bacteriology reporting and information system. Acta Pathol Microbiol Immunol Scand [B] 1984; 92: 119–126.
6. Blair JE, Williams REO. Phage typing of staphylococci. Bull WHO 1961; 24: 771–784.
7. de Lencastre H, Chung M, Westh H. Archaic strains of methicillin-resistant Staphylococcus aureus: molecular and microbiological properties of isolates from the 1960s in Denmark. Microb Drug Resist 2000; 6: 1–10.
8. Tenover FC, Arbeit RD, Goering RV, Mickelsen PA, Murray BE, Persing DH, et al. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol 1995; 33: 2233–2239.
9. Shopsin B, Gomez M, Montgomery SO, Smith DH, Waddington M, Dodge DE, et al. Evaluation of protein A gene polymorphic region DNA sequencing for typing of Staphylococcus aureus strains. J Clin Microbiol 1999; 37: 3556–3563.
10. Harmsen D, Claus H, Witte W, Rothganger J, Turnwald D, Vogel U. Typing of methicillin-resistant Staphylococcus aureus in a university hospital setting by using novel software for spa repeat determination and database management. J Clin Microbiol 2003; 41: 5442–5448.
11. Tenover FC, Arbeit R, Archer G, Biddle J, Byrne S, Goering R, et al. Comparison of traditional and molecular methods of typing isolates of Staphylococcus aureus. J Clin Microbiol 1994; 32: 407–415.
12. Breuer K, HAussler S, Kapp A, Werfel T. Staphylococcus aureus: colonizing features and influence of an antibacterial treatment in adults with atopic dermatitis. Br J Dermatol 2002; 147: 55–61.
13. Hoeger PH, Lenz W, Boutonnier A, Fournier JM. Staphylococcal skin colonization in children with atopic dermatitis: prevalence, persistence, and transmission of toxigenic and nontoxigenic strains. J Infect Dis 1992; 165: 1064–1068.
14. Balslev U, Bremmelgaard A, Svejgaard E, Havstreym J, Westh H. An outbreak of borderline oxacillin-resistant Staphylococcus aureus (BORSA) in a dermatological unit. Microb Drug Resist 2005; 11: 78–81.
15. Thauvin-Eliopoulos C, Rice LB, Eliopoulos GM, Moellering RC Jr. Efficacy of oxacillin and ampicillin-sulbactam combination in experimental endocarditis caused by beta-lactamase-hyperproducing Staphylococcus aureus. Antimicrob Agents Chemother 1990; 34: 728–732.
16. Kline MW, Mason EO Jr, Kaplan SL. Outcome of heteroresistant Staphylococcus aureus infections in children. J Infect Dis 1987; 156: 205–208.
17. Massanari RM, Pfaller MA, Wakefield DS, Hammons GT, McNutt LA, Woolson RF, et al. Implications of acquired oxacillin resistance in the management and control of Staphylococcus aureus infections. J Infect Dis 1988; 158: 702–709.

