


Shiro Niiyama1, Shinsaku Aiba1, Kensei Katsuoka1, Yoshinori Ito2 and Noriyoshi Sumiya2
1Department of Dermatology, Kitasato University, and 2Department of Plastic and Reconstructive Surgery, Fujigaoka Hospital, Showa University School of Medicine, Kanagawa, Japan
Numerous surgical methods have been introduced to treat osmidrosis. However, many problems with wound healing have been reported, including haematoma, seroma, skin necrosis and severe scarring. Ultrasound energy liquefies sweat glands via cavitation, but minimally affects blood vessels and nerves at the same energy level. Our patient was treated with ultrasonic surgical aspiration, which allowed the effective removal of the apocrine glands with little scarring. The ultrasonic surgical aspirator offers a safe and effective method to treat osmidrosis with few complications. This is the operation of first choice, especially for the patients who are sensitive about their surgical scars. Key words: axillary apocrine glands; osmidrosis; ultrasonic aspiration.
(Accepted January 4, 2006.)
Acta Derm Venereol 2006; 86: 238–240.
Shiro Niiyama, Department of Dermatology, Kitasato University, 1-15-1 Kitasato, Sagamihara, Kanagawa, 228-8555 Japan. E-mail: sniiyama@aol.com
The characteristic of axillary osmidrosis is usually excessive malodour, which adversely affects patients’ social and personal life. It is generally agreed that the odour originates from bacterial decomposition of sweat secreted from apocrine glands (1). Compared with individuals not suffering from osmidrosis, an increase in the ratio of apocrine to eccrine glands has been reported (2).
The ultrasonic surgical aspirator has long been used in renal surgery (3), neurosurgery (4) and plastic surgery (5, 6), and is widely available in hospital settings. The ultrasound-assisted apocrine gland aspiration method was introduced by Chung and colleagues (7). The ultrasonic energy caused cavitation in high fluid content tissues, such as sweat glands, resulting in liquefaction and subsequent removal by suction. But at the same energy level, solid adjacent structures such as blood vessels and nerves were minimally affected.
We report here a relatively simple method using ultrasonic surgical aspiration for removal of axillary apocrine sweat glands for treating an individual with osmidrosis. The measures used to manage postoperative sequelae are also described.
CASE REPORT and methods
An 18-year-old woman with osmidrosis axillae had received treatments with various external preparations for approximately 3 years. All these treatments were, however, ineffective. The degree of osmidrosis axillae is classified at our institution into 5 grades, obtained using gauze held under the patient’s arm for 1 min: grade 0: the gauze is not malodorous; grade 1: the gauze is slightly malodorous (when carefully sniffing the gauze); grade 2: the gauze is malodorous (with the gauze immediately in front of the face); grade 3: the gauze is strongly malodorous (can be smelt when holding the gauze away from the face); and grade 4: the axillae are malodorous and can be smelt even before the gauze is held under the patient’s arm. Our patient’s condition was classified as grade 4. Based on these observations, surgical treatment was chosen for this patient.
The ultrasonic surgical aspirator used for this treatment is the Sumisonic ME-2400 (Sumitomobakelite, Tokyo, Japan). The aspirator is composed of a main unit and a handpiece. The tip of the handpiece is made of titanium and has a 2 mm diameter, 28 kHz frequency, and 300 µm maximum oscillation. The operator can adjust the level of oscillation between 0 and 100. The area around the tip is irrigated with physiological saline, which is suctioned away through the tip.
This patient was placed in a supine position with her arms abducted from the trunk to approximately 100° in order to expose the axilla and to avoid injury to the brachial plexus. Markings were made around the location of the axillary hair-bearing area, where the apocrine glands are thought to be located. A local infiltration anaesthesia was administered. While waiting for the effect of local anaesthesia, the ultrasonic aspirator was set up. The ultrasonic power was set at 60% and the rate of saline irrigation was set at 30 ml/min. A 2 cm incision was made in the parallel direction of the axillary crease on the central portion of the hair-bearing axillary area. To maintain neurovascular bundles, undermining was performed parallel to the subdermal plexus with Metzenbaum scissors. While holding the handpiece like a pen, the operator lightly pressed the tip onto the undersurface of the axillary skin and moved it around in continuous circular, brush-like motions (Fig. 1). The ultrasound energy emitted from the titanium tip resulted in cavitation and subsequent fragmentation of the sweat glands, and the suction allowed for removal of the liquefied sweat glands. Effective removal of apocrine glands was demonstrated by the appearance of hair follicles and dermis. Histological examination of specimens showed elimination of the apocrine glands (Fig. 2). Wounds were closed with sutures, followed by coverage with compressive bandages for 3 days. Sutures were removed approximately 10 days after surgery, and active shoulder movements were prohibited for 2 weeks postoperatively. Two weeks postoperatively the patient’s osmidrosis axillae was evaluated as grade 0. There has been no recurrence in the 3 postoperative months to date.

Fig. 1. Inserting the handpiece through the incision.
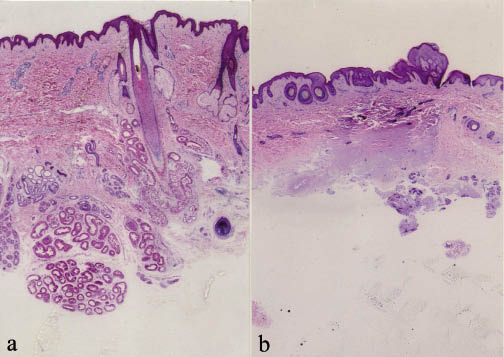
Fig. 2. Histological appearance. (a) Before ultrasonic aspiration. Normal axillary skin architecture showing apocrine glands. (b) After ultrasonic aspiration. The apocrine glands have been removed. (H&E, original magnification ×40).
DISCUSSION
Osmidrosis is a common condition usually managed by regular showering and use of commercially available antiperspirants or deodorants. However, in some individuals conventional methods are not effective at controlling the foul odour. To treat such severe cases, various types of surgical methods have been introduced (8–11). Of these procedures, manual shaving had the lowest recurrence rate for malodour (12). Carbon dioxide laser vapourization had results similar to manual shaving except for a clinically higher recurrence rate (12). Liposuction had advantages, such as small invisible scars, a short-term immobilization period, and the least number of surgical complications, but it had a high rate of dissatisfaction in postoperative malodour (12). Therefore, removal of subcutaneous apocrine glands by manual subdermal shaving is the preferred method. However, many problems with wound healing have been reported: haematoma, seroma, skin necrosis and severe scarring. Contracture and irregular axillary hair loss were frequent long-term results. The use of bulky and uncomfortable dressings for up to several weeks was also routine and disliked by many patients.
The use of an ultrasonic aspirator allowed us to remove apocrine glands with less scarring. The ultrasonic energy caused cavitation in high fluid content tissues such as sweat glands. The cavitation is followed by blasting and liquefaction of apocrine glands. As such, ultrasound energy is more effective within apocrine glands, since this tissue is less dense than more cohesive tissues such as blood vessels, nerves and muscle. Therefore, it offers the advantages of fairly effortless removal of apocrine glands, with less bleeding, due to minimal destruction of more solid tissue such as blood vessels (13). It contributes preservation of circulation to the axilla skin and we have not seen any wound healing problems, contractures or noticeable axillary hair loss. However, even though the ultrasonic surgical aspirator seems to offer a safer way to treat osmidrosis, it still should be used with care to avoid potential complications such as skin necrosis via a thermal effect. Burns can occur if the operator presses too hard or the device is allowed to remain stationary. However, this problem can be avoided simply by moving the handpiece tip across the undersurface of the axillary skin with small, uninterrupted, brush-like strokes. In our clinic, the axillae are cooled by irrigation with saline maintained at 4°C throughout the operation. Topical steroids are applied to the affected area for a few days postoperatively to prevent burn reactions. The ultrasonic surgical aspirator offers an option that is relatively simple, safe and effective method with few complications. This is the operation of first choice, especially for patients who are sensitive about their surgical scars.
REFERENCES
1. Leyden JJ, McGinley KJ, Hölzle E, Labows JN, Kligman AM. The microbiology of the human axilla and its relationship to axillary odor. J Invest Dermatol 1981; 77: 413–416.
2. Bang YH, Kim JH, Paik SW, Park SH, Jackson IT, Lebeda R. Histopathology of apocrine bromhidrosis. Plast Reconstr Surg 1996; 98: 288–292.
3. Chopp RT, Shah BB, Addonizio JC. Use of ultrasonic surgical aspirator in renal surgery. Urology 1983; 22: 157–159.
4. Flamm ES, Ransohoff J, Wuchinich D, Broadwin A. Preliminary experience with ultrasonic aspiration in neurosurgery. Neurosurgery 1978; 2: 240–245.
5. Ito Y, Kondo S, Sumiya N, Yoshii M, Otani K, Wako M. Dermabrasion using an ultrasonic surgical aspirator. Plast Reconstr Surg 1996; 97: 1034–1039.
6. Otani K, Ito Y, Sumiya N, Kondo S, Ieba S. Treatment of Bowen disease using the ultrasonic surgical aspirator. Plast Reconstr Surg 2001; 108: 68–72.
7. Chung S, Yoo WM, Park YG, Shin KS, Park BY. Ultrasonic surgical aspiration with endoscopic confirmation for osmidrosis. Br J Plast Surg 2000; 53: 212–214.
8. Yoshikata R, Yanai A, Takei T, Shionome H. Surgical treatment of axillary osmidrosis. Br J Plast Surg 1990; 43: 483–485.
9. Park JH, Cha SH, Park SD. Carbon dioxide laser treatment vs subcutaneous resection of axillary osmidrosis. Dermatol Surg 1997; 23: 247–251.
10. Ou LF, Yan RS, Chen IC, Tang YW. Treatment of axillary bromhidrosis with superficial liposuction. Plast Reconstr Surg 1998; 102: 1479–1484.
11. Jemec B. Abrasio axillae in hyperhidrosis. Scand J Plast Reconstr Surg 1975; 9: 44–46.
12. Park YJ, Shin MS. What is the best method for treating osmidrosis? Ann Plast Surg 2001; 47: 303–309.
13. Zocchi ML. Ultrasonic assisted lipoplasty: technical refinements and clinical evaluations. Clin Plast Surg 1996; 23: 575–598.

