


Eugenia Mayo-Pampín, Ángeles Flórez, Carlos Feal, Alberto Conde, María Teresa Abalde, Carlos De la Torre, Ignacio Doval and Manuel J Cruces
Department of Dermatology, Hospital Provincial Pontevedra, C/ Loureiro Crespo 2, ES-36001 Pontevedra, Spain. E-mail: emaypam@aedv.es
Accepted March 21, 2006
Sir,
Acute generalized exanthematous pustulosis (AGEP) is a cutaneous reaction characterized by an acute non-follicular pustular eruption overlying a scarlatiniform background, usually associated with high fever and neutrophilia. This rare disease is generally drug-induced, particularly by antibacterial drugs. Only two other cases provoked by pseudoephedrine ingestion have been reported. Patch testing has been advocated recently as a potentially useful test in patients with AGEP.
We report here a case of pseudoephedrine-induced AGEP where subsequent patch testing results were positive.
CASE REPORT
A 41-year-old man was admitted for evaluation of an acute, tender, erythematous and pustular eruption accompanied by fever and malaise. Cutaneous lesions had begun in the antecubital, inguinal and popliteal folds, quickly spreading to involve the entire body. Twenty-four hours previously the patient had ingested one tablet of Rinoebastel® (ebastine 10 mg, pseudoephedrine 120 mg) to treat nasal discharge. The patient was otherwise healthy, and had no personal or family history of psoriasis or other skin disease.
Clinical examination revealed fever (38.2ºC), bilateral tender cervical, axillar and inguinal adenopathies, and generalized scarlatiniform erythema scattered with multiple non-follicular pustules and intense facial oedema. Palmar and plantar areas were spared. The inferior lip semi-mucose was erythematous and eroded. There was no evidence of other mucous membrane involvement (Fig. 1).
Fig. 1. Erythematous rash covered with non-follicular pustules.

Laboratory studies including blood cell count, liver and renal function test and electrolytes were all within normal limits except from leukocytosis 21.3×109/l (4.5–11×109/l) with neutrophilia 87% (40–75%). Chest radiogram and abdominal ultrasonography were normal. Bacterial cultures from the throat and pustules produced negative results. Serological tests for HIV, cytomegalovirus, Epstein-Barr virus, hepatitis B and C, Coxsackie and Treponema pallidum were all negative.
A cutaneous biopsy showed subcorneal non-follicular pustules, epidermal spongiosis, focal keratinocytic necrosis and basal vacuolar degeneration. Papillary dermal oedema and diffuse perivascular infiltrates of neutrophils, eosinophils and lymphocytes were present in the superficial dermis. No bacterial or fungal organisms were identified.
Patch tests showed an intense positive result (++++) at 48 and 96 h with the commercial preparation Rinoebastel® 2,5% and 5% in petrolatum, as well as with pseudoephedrine 1% in petrolatum. Epicutaneous tests with ebastine 1% and 2% in petrolatum were negative (Fig. 2). The results of patch testing were reported according to the International Contact Dermatitis Research Group criteria for patch test reading.
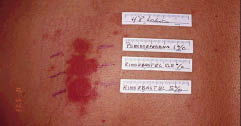
Fig. 2. Patch test positive with pseudoephedrine 1%, Rinoebastel® 2.5% and 5% in petrolatum coat.
Total resolution was observed within 7 days without specific treatment, followed by intense desquamation. The patient was instructed not to ingest drugs containing pseudoephedrine.
DISCUSSION
AGEP was first coined as an entity by Beylot et al. in 1980 (1). Today the disease is an uncommon, although well-known clinical entity, characterized by acute onset and rapid self-healing course, fever, leukocytosis and widespread, sterile, non-follicular pin-head pustules on an erythematous background. Histological examination reveals non-follicular subcorneal pustules generally associated with dermal oedema, perivascular inflammation and focal keratinocytic necrosis (2).
The main differential diagnosis of a generalized pustular eruption with fever include acute pustular psoriasis von Zumbusch type, pustulosis acuta generalisata (post-streptococcal disease arising mainly in children), drug hypersensitivity syndrome, toxic epidermal necrolysis, Sneddon-Wilkinson subcorneal pustular dermatosis and pustular vasculitis.
AGEP is generally a drug-induced disease. During the last 10 years several drugs, particularly antibiotics such as aminopenicillins and macrolides have been reported as being responsible of causing AGEP (3, 4). Other aetiological factors reported so far include viral infections (enterovirus or parvovirus B19), cystic echinococcosis, ingestion of chromium picolinate, lacquer chicken, contact hypersensitivity to mercury (2) and exposure to ultraviolet radiation (5).
The exact pathomechanism of AGEP is currently unknown. Although initially it was considered a type III hypersensitivity reaction, today most authors defend a type IV delayed hypersensitivity reaction. Positive skin patch test results and short time between introduction of the drug and onset of the eruption support this hypothesis (2). Padial et al. confirmed the presence of a perivascular T-cell infiltrate composed mainly of proliferating activated memory lymphocytes in addition to the polymorphonuclear cells and the increase in the local production of IL-8 in the skin (6).
Patch testing is nowadays a generally accepted tool in the search for the causative agent of AGEP (6, 7), especially since oral rechallenge may provoke a generalized eruption, even at a low dose. Patch testing is a good alternative to prove the causative role of a suspected drug and it is particularly useful when there are several potential causative drugs. Beylot et al. (8) Wolkestein et al. (9) and Watsky (10) have reported positive patch test results in approximately 50% of AGEP cases (2, 8). Despite their lack of sensitivity, a negative test result cannot definitely exclude a sensitization to the substance tested (9). Recently, Mashiah & Brenner (7) reported a case of AGEP provoked by a patch test with acetaminophen. Interestingly, patch test results obtained with the offending drug were negative. The authors reported possible explanations to this negative results: low concentration of the drug being tested, insufficient amount of the drug applied, inappropriate vehicle, degradation of the substance and UV radiation of the patch test site (7).
Pseudoephedrine is a decongestant prescribed to relieve nasal discomfort caused by colds, allergies and hay fever. Side-effects from pseudoephedrine are uncommon. To our knowledge, only two previous similar cases of AGEP due to pseudoephedrine have been reported until now (6, 11).
REFERENCES
1. Beylot C, Bioulac P, Doutre MS. Acute generalized exanthematic pustuloses (four cases). Ann Dermatol Venereol 1980; 107: 37–48.
2. Machet L, Martin L, Vaillant L. Acute generalized exanthematic pustulosis. Ann Dermatol Venereol 2001; 128: 73–79.
3. Haro-Gabaldon V, Sanchez-Sanchez-Vizcaino J, Ruiz-Avila P, Gutierrez-Fernandez J, Linares J, Naranjo-Sintes R. Acute generalized exanthematous pustulosis with cytomegalovirus infection. Int J Dermatol 1996; 35: 735–737.
4. Young PC, Turiansky GW, Bonner MW, Benson PM. Acute generalized exanthematous pustulosis induced by chromium picolinate. J Am Acad Dermatol 1999; 41: 820–823.
5. Yip J, Sheehan-Dare R, Cotterill J. Toxic pustuloderma due to PUVA treatment. Br J Dermatol 1991; 125: 401–402.
6. Padial MA, Alvarez-Ferreira J, Tapia B, Blanco R, Manas C, Blanca M, et al. Acute generalized exanthematous pustulosis associated with pseudoephedrine. Br J Dermatol 2004; 150: 139–142.
7. Mashiah J, Brenner S. A systemic reaction to patch testing for the evaluation of acute generalized exanthematous pustulosis. Arch Dermatol 2003; 139: 1181–1183.
8. Beylot C, Doutre MS, Beylot-Barry M. Acute generalized exanthematous pustulosis. Semin Cutan Med Surg 1996; 15: 244–249.
9. Wolkenstein P, Chosidow O, Flechet ML, Robbiola O, Paul M, Dume L, et al. Patch testing in severe cutaneous adverse drug reactions, including Stevens-Johnson syndrome and toxic epidermal necrolysis. Contact Dermatitis 1996; 35: 234–236.
10. Watsky KL. Acute generalized exanthematous pustulosis induced by metronidazole: the role of patch testing. Arch Dermatol 1999; 135: 93–94.
11. Assier-Bonnet H, Viguier M, Dubertret L, Revuz J, Roujeau JC. Severe adverse drug reactions due to pseudoephedrine from over-the-counter medications. Contact Dermatitis 2002; 47: 165–182.

