


Reflections after the first year on our own
One year ago I announced that we would end our collaboration with a commercial publisher as of January 2006 and start to publish Acta Dermato-Venereologica by ourselves. The non-profit organization who owns the journal, The Society for Publication of Acta Dermato-Venereologica, had several reasons for making this decision: first, our prognostic calculations showed that the journal’s economic situation would improve by such a change; second, we wanted the journal to move more quickly towards open access and to ascertain that all steps in the publication process adhered to a non-profit ideology.
Have all these goals been fulfilled? Yes, the economy has changed from deficits over the last 5 years to a small surplus for 2006. Thanks to a generous grant from the Welander-Finsen Foundation covering some of the accumulated deficits we are now in a healthy (non profit!) situation. Meanwhile open access after 1 year has been instituted for all papers with a possibility for immediate open access for selected papers (reviews, high impact papers, etc.). This is a first step towards total open access; however before this is fully executed we must know better how to balance the expected fall in subscription income against the need for additional page charges. So far the shift of the Acta Dermato-Venereologica’s policy from a commercial publisher to publication in its own right has been surprisingly smooth and successful, which is most certainly due to our extremely competent and efficient editorial manager, Mrs Agneta Andersson, and her team of co-workers at the editorial office.
By all these changes we are convinced that Acta Dermato-Venereologica will continue to receive numerous high-quality submissions from investigators around the world and to attract the interest of plenty readers, hopefully resulting in a further increase of the impact factor, presently being 1.741 (Fig. 1).
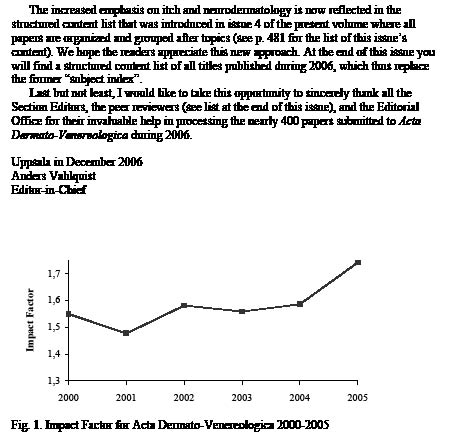
Fig. 1. Impact Factor for Acta Dermato-Venereologica 2000-2005
New section editors and new approaches
I am happy to welcome 3 new Section Editors who are working for our journal since the fall of 2006: Dr Elke Weisshaar, Associate Professor Håkan Mobacken and Professor Earl Carstens.
Håkan Mobacken, Gothenburg University, will take over the clinical case reports from Dr Flemming Brandrup, Odense, who will leave the Board in 2007 due to other commitments after having done 3 years of fantastic work as Section Editor. We are very grateful for all his efforts during this time. Dr Mobacken is a leading Clinical Dermatologists in Sweden; his experience and working capacity indeed bring new competence to our journal.
Elke Weisshaar, Heidelberg, and Earl Carstens, San Francisco, will share the responsibility for all submitted papers related to itch, which no doubt is one of the most problematic symptoms in Dermatology. Professor Carstens is a leading expert in the neurophysiology of itch, and Dr Weisshaar is a Clinical Dermatologist who has long-standing experience in the research on itch and its therapy. Their joining the Editorial Board not only brings new, outstanding expertise in the field of itch, but also represents a milestone in raising the scientific status of itch and neurodermatology in the dermatologic literature.
The increased emphasis on itch and neurodermatology is also reflected in the structured content list that was introduced in issue 4 of the present volume where all papers are organized and grouped after topics (see p. 481 for the list of this issue’s content). We hope the readers appreciate this new approach. At the end of this issue you will find a structured content list of all titles published during 2006, which thus replaces the former “subject index”.
Last but not least, I would like to express my sincere thanks to all the Section Editors, the peer reviewers (see list at the end of this issue), and the Editorial Office for their invaluable help in processing the nearly 400 papers submitted to Acta Dermato-Venereologica during 2006.
Uppsala in November 2006
Anders Vahlquist
Editor-in-Chief
In Forsberg S, Saarialho-Kere U, Rollman O. Comparison of Growth-inhibitory Agents by Fluorescence Imaging of Human Skin Re-epithelialization In vitro. Acta Derm Venereol 2006; 86: 292–299 Table I is incorrect. The correct table is as follows:
Table I. Estimated radial growth rates (µm/day) for drugs tested at three different concentrations. Mean values±SEM from three independent experiments are given. n=12 for each group
| 1 µM | 100 nM | 10 nM | ||||
| Drug | Growth rate | pa | Growth rate | pa | Growth rate | pa |
| PKI166 | 393±9 | <0.0001 | 466±8 | 0.168 | 475±5 | 0.459 |
| Calcipotriol | 411±16 | <0.0001 | 495±15 | 0.419 | 510±9 | 0.051 |
| Betamethasone | 456±12 | 0.033 | 459±8 | 0.054 | 478±10 | 0.625 |
| Tacrolimus | 470±15 | 0.274 | 457±9 | 0.035 | 460±12 | 0.064 |
| Dithranol | 486±12 | 0.932 | 476±10 | 0.494 | 482±13 | 0.848 |
| Tazarotene | 517±13 | 0.015 | 501±11 | 0.209 | 501±11 | 0.223 |
| Vehicle | 485±7 | |||||
aStatistical test of difference in radial growth rate between drug and vehicle as described in the materials and methods section.
In Halvorsen JA, Brevig T, Aas T, Skar AG, Slevolden EM, Moi H. Genital Ulcers as Initial Manifestation of Epstein-Barr Virus Infection: Two New Cases and a Review of the Literature. Acta Derm Venereol 2006; 86: 439–442 Table I is incorrect. The correct table is as follows:
Also the sentence in Case 2, first paragraph ”She received benzyl penicillin for tonsillitis...”, is incorrect. The correct sentence is as follows: ”She received phenoxymethylpenicillin for tonsillitis...”
Table I. Serological findings in two cases of probable Epstein-Barr-virus-associated genital ulcers
| Genital ulcer(s) appeared | VCA-IgM neg VCA-IgG neg EBNA-IgG neg | VCA-IgM pos VCA-IgG neg EBNA-IgG neg | VCA-IgM neg VCA-IgG pos EBNA-IgG pos | Negative for HSV, CMV, TP, Hep B and HIV | |
| Case 1 | Day 1 | Day 3 | Day 13 | 6 months | 6 months |
| Case 2 | Day 1 | ND | Day 9 | 6 months | 6 months |
VCA-IgM, IgM antibodies to EBV capsid antigen; VCA-IgG, IgG antibodies to EBV capsid antigen; EBNA-IgG, IgG antibodies to Epstein-Barr nuclear antigen; HSV, IgG to herpes simplex virus; CMV, cytomegalovirus antibodies, TP, Treponema pallidum antibodies; HIV, human immunodeficiency virus; Hep B, hepatitis B serology; ND, not done.

