Nádia Barbosa Aires, Mírian N. Sotto and Marcello M. S. Nico
Department of Dermatology, University of São Paulo Medical School, São Paulo, Brazil



Nádia Barbosa Aires, Mírian N. Sotto and Marcello M. S. Nico
Department of Dermatology, University of São Paulo Medical School, São Paulo, Brazil
Nephrogenic fibrosing dermopathy is a recently described fibrosing disorder that emerges in different settings of renal insufficiency. The degree and cause of the underlying renal impairment seem not to be related to the severity of the nephrogenic fibrosing dermopathy. Lesions are typically symmetrical and usually develop on the limbs and trunk. These are characterized by skin-coloured to erythematous papules that coalesce into plaques markedly thickened in texture. Flexion contractures of the joints may be a feature of the disease. There is no consistently effective therapy for nephrogenic fibrosing dermopathy. We report here 2 Brazilian patients in connection with a short review. Remission was recorded in one case after plasmapheresis. Key words: nephrogenic fibrosing dermopathy; scleromyxoedema-like cutaneous disease; kidney transplantation.
(Accepted March 12, 2007.)
Acta Derm Venereol 2007; 87: 521–524.
Nádia Barbosa Aires, Rua Oscar Freire, 2040 ap 172, São Paulo SP, CEP-05409-011, Brazil. E–mail: nadiaaires@yahoo.com.br
Nephrogenic fibrosing dermopathy (NFD) is a recently described, acquired, idiopathic entity (1, 2). This condition was first observed in 1997 and reported as a scleromyxoedema-like disorder in 2000 (3). To date, the registry for NFD lists approximately 175 cases worldwide and its incidence is increasing as new cases are continuously reported (3–5).
The primary lesions are skin-coloured to erythematous papules that coalesce into plaques with irregular projections, which are hard on palpation (2, 5–11). The lesions are typically symmetrical (5–8) and the face is usually spared (2, 7, 8).
Disease activity in NFD seems to parallel renal function (4, 6, 12). The return of normal renal function usually results in an improvement, but it does not guarantee the resolution of NFD (4, 6, 12, 13). The cause of NFD remains unknown (3, 6, 14).
CASE REPORTS
Case 1
A 23-year-old woman had been treated with haemodialysis for 5 years because of renal insufficiency due to polycystic kidney disease. She received a live-donor renal transplantation, but developed an acute renal insufficiency caused by rejection of the graft, which was treated with methylprednisolone. Additional treatment with cyclosporin A, azathioprine and mycophenolate mofetil was given. Four months after the transplantation, she presented with anasarca followed by appearance of erythematous papules on the inner side of the thighs, on the forearms and the hands, which coalesced into plaques leading to a sclerotic and cicatricial appearance (Fig. 1A and B). Palmar lesions were incapacitating, leading to pain and inability to close the fist. Skin biopsy revealed a mild dermal proliferation of fibroblasts, thick collagen bundles and an increase in dermal mucin (Fig. 2A). The irregular dermal collagen bundles were surrounded by CD34-positive dermal dendrocytes (Fig. 2B). After 3 months, the rejection process was controlled, followed by normalization of the renal function and spontaneous improvement of the cutaneous lesions. She had no paraprotein and was negative for antinuclear antibodies (ANA).
Case 2
A 24-year-old woman presented with chronic renal insufficiency of unknown cause for 2 years, which was treated with peritoneal dialysis. After 2 years she received a renal transplant from a living donor, which was lost because of arterial thrombosis in the immediate post-operative period. Simultaneously, she presented with bilateral iliac vein thrombosis treated with anticoagulants. Peritoneal dialysis was reinstituted, followed by haemodialysis. At this moment anasarca developed, followed by appearance of thickened, erythematous to brownish plaques leading to a sclerotic and cicatricial area on the dorsal side of the legs, thighs, buttocks and arms (Fig. 1C).

Fig. 1. (A) Brownish plaques on the dorsal side of the forearms of case 1. (B) Palmar lesions with diffuse infiltration sparing the palmar crests in case 1. (C) Erythematous and squamous plaques on the buttocks of case 2.
Histopathological study of the lesions revealed fibrosis in the upper dermis and increased deposits of mucin. Immunostaining revealed dermal dendrocytes positive to CD34 and clefts of factor XIIIa positive cells (Fig. 2C).
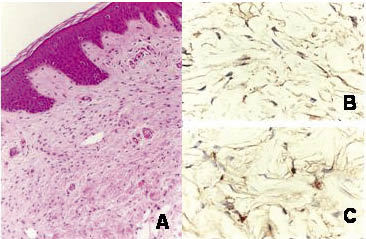
Fig. 2. Diagnostic study of case 2.
(A) Thickened dermis with prominent spindle cells among collagen tissue (skin biopsy from buttock; (H&E ×200 original magnification).
(B) CD34-positive dendrocytes intermingled between coarse collagen tracts (anti-CD34 antibody, immunohistochemical technique; ×400 original magnification).
(C) Factor XIIIa positive dendrocytes in reticular dermis (anti-XIIIa factor antibody; immunohistochemical technique; ×400 original magnification).
She was treated with 6 sessions of plasmapheresis, 3 times a week, in a MCS 980E equipment (Haemonetics MCS+ 9000, Haemonetics Corporation, Massachussets, MA, USA) with exchange of 2000 ml (40 ml/kg) of serum for the same volume of 4% albumin in each session, without any adverse effects. There was gradual improvement in the texture and dimension of the skin lesions. After one year of follow-up there were no active lesions and no new plaques.
DISCUSSION
NFD is an uncommon entity that affects end-stage renal disease and patients on dialysis; the aetiology is unknown (1, 3, 15). Its abrupt appearance suggests that toxic exposures or infectious agents may be involved in the aetiopathogenesis of the disease (6, 15–18). Until now, no such agent has been identified (11). Other hypotheses have been proposed, such as anti-cardiolipin antibodies, vascular injury or circulating fibrocytes as part of the pathogenesis (6, 14).
Our patients had in common end-stage renal insufficiency, renal allograft transplantation, haemodialysis, vascular complications and severe oedema preceding the cutaneous lesions. All of these could be a triggering agent to this new entity, as was suggested.
Recent investigations suggest that a recently characterized cell involved in wound healing, the circulating fibrocyte, might be implicated in the pathogenesis of NFD. This cell has a CD34/procollagen dual-positive profile and is thought to leave the circulation and differentiate in the dermis into cells that resemble normal dermal fibroblasts. However, this hypothesis has not been established with certainty (3, 5, 6, 12). Due to the presence of these circulating cells, NFD might be considered a systemic disorder that is supported by the symmetry of the lesions, rapid development of the disease at different sites, and the close resemblance of the cellular composition of NFD to a wound-healing reaction. The resolved lesions of NFD are indistinguishable from those of a healed wound (13, 19). Other aspects that suggest systemic involvement include reports of concomitant cardiomyopathy, pulmonary fibrosis, fibrotic infiltration of the diaphragm and psoas muscle, kidney and rete testes fibrosis, which were not found in our patients (10, 20, 21).
It is possible that the noxious causative agent induces an increased expression of TGF-β by the dendritic cells that would be responsible for the fibrotic process (10). Histopathology of the early lesions (< 20 weeks after clinical onset) exhibit large epithelioid or stellate spindle cells in the reticular dermis that can extend into and widen the septa of subcutaneous fat lobules. The reticular dermal collagen bundles are thickened with surrounding clefts that are interposed by CD34-positive dendritic cells (11, 17). The lesions show variable amounts of dermal mucin (7, 11). Inflammatory cells are usually absent (11). These findings are similar to the observations in our patients.
Advanced lesions (> 20 weeks after clinical onset) typically have large collagen bundles, but the clefts are less prominent and often thinner (11); less mucin, and fewer CD34 positive dendritic cells are found (7, 11). The majority of spindle cells reveal strong cytoplasmic CD34 immunostaining that highlights their dendritic processes. This feature was encountered in our patients (3, 22, 23).
There is no single pathognomonic test for the diagnosis of NFD (6). The characteristic morphology and distribution of cutaneous involvement, associated with the histological findings, in the context of a patient with underlying renal disease is unique, and allows the diagnosis (5, 7, 14). Nevertheless, there are some other fibrosing entities that must be differentiated from NFD. The main differential diagnoses are scleromyxoedema, systemic sclerosis, eosinophilic fasciitis, eosinophilia-myalgia syndrome and Spanish toxic oil syndrome (7, 11, 15).
To date, there is no consistently effective therapy for NFD. Many treatments have been proposed, such as plasmapheresis, photopheresis, thalidomide, high oral doses of corticosteroids, high-dose intravenous immunoglobulin, cyclosporine, tacrolimus, topical psoralen plus ultraviolet A, topical steroids, mycophenolate mofetil, calcipotriene ointment, cyclophosphamide, and physical therapy (5, 6, 8, 13, 14, 18, 23–28).
The first case described in this paper showed spontaneous remission of the lesions after normalization of renal function. The second case was treated with plasmapheresis according to previous successful results (23). Plasmapheresis is supposed to reduce the levels of plasmatic TGF-β, thus blocking the pathophysiology of the disease (14, 23). The patient was treated with 6 sessions of plasmapheresis and obtained gradual improvement in the size and texture of the lesions.
Other authors obtained improvement in NFD after transplantation and subsequent normalization of renal function (12, 23, 25). Because many patients with NFD present an underlying thrombotic tendency, a careful hypercoagulation work-up should precede any surgery, and precautions should be taken to avoid thrombotic loss of the new renal graft (12).
The 2 patients studied by us are the only 2 cases that developed NFD among a cohort of 3019 kidney allografted patients treated in our medical institution since 1965. Awareness of this new entity may improve accuracy of diagnosis in other kidney disease centres.
REFERENCES
1. Gambichler T, Paech V, Kreuter A, Wilmert M, Altmeyer P, Stucker M. Nephrogenic fibrosing dermopathy. Clin Exp Dermatol 2004, 29: 258–260.
2. Cowper SE, Robin HS, Steinberg SM, Su LD, Gupta S, LeBoit PE. Scleromyxoedema-like cutaneous disease in renal-dialysis patients. Lancet 2000; 356: 1000–1001.
3. Swaminathan S, Leung N. Nephrogenic fibrosing dermopathy: lessons from the past. Int J Dermatol 2006; 45: 639–641.
4. Cowper SE, Bucala R, LeBoit PE. Case 35-2004: nephrogenic fibrosing dermopathy. N Engl J Med 2005; 352: 1723–1724.
5. Cowper SE. Nephrogenic fibrosing dermopathy [NFD/NSF Website]. 2001–2005. Available from: http://www.icnfdr.org. Accessed 07/04/2006.
6. Cowper SE. Nephrogenic fibrosing dermopathy: the first 6 years. Curr Opin Rheumatol 2003; 15: 785–790.
7. Streams BN, Liu V, Liegeois N, Moschella SM. Clinical and pathologic features of nephrogenic fibrosing dermopathy: a report of two cases. J Am Acad Dermatol 2003; 48: 42–47.
8. Evenepoel P, Zeegers M, Segaert S, Claes K, Kuypers D, Maes B, et al. Nephrogenic fibrosing dermopathy: a novel, disabling disorder in patients with renal failure. Nephrol Dial Transplant 2004; 19: 469–473.
9. Markus JS, James AJ, Nunez-Gussman JK, Sheehan AM, Fegan L, Hsu S. Nephrogenic fibrosing dermopathy. J Am Acad Dermatol 2005; 52: 166–167.
10. Jimenez SA, Artlett CM, Sandorfi N, Derk C, Latinis K, Sawaya H, et al. Dialysis-associated systemic fibrosis (nephrogenic fibrosing dermopathy) study of inflammatory cells and transforming growth factor β1 expression in affected skin. Arthrit Rheum 2004; 50: 2660–2666.
11. Ishibe S, Perazella MA, Reilly RF. Nephrogenic fibrosing dermopathy: an unusual skin condition associated with kidney disease. Semin Dialysis 2003; 16: 276–280.
12. Cowper SE. Nephrogenic systemic fibrosis: the nosological and conceptual evolution of nephrogenic fibrosing dermopathy. Am J Kidney Dis 2005; 46: 763–765.
13. Gilliet M, Cozzio A, Burg G, Nestle FO. Successful treatment of three cases of nephrogenic fibrosing dermopathy with extracorporeal photopheresis. Br J Dermatol 2005; 152: 531–536.
14. Mackay-Wiggan JM, Cohen DJ, Hardy MA, Knobler EH, Grossman ME. Nephrogenic fibrosing dermopathy (scleromyxedema-like illness of renal disease). J Am Acad Dermatol 2003; 48: 55–60.
15. Cowper SE, Su LD, Bhawan J, Robin HS, LeBoit PE. Nephrogenic fibrosing dermopathy. Am J Dermatopathol 2001; 23: 383–393.
16. Dawn G, Holmes SC.Scleromyxoedema-like eruption following haemodialysis or nephrogenic fibrosing dermopathy? Br J Dermatol 2004; 150: 155–177.
17. Neudecker BA, Stern R, Mark LA, Steinber S. Scleromyxoedema-like lesions of a patient in renal failure contain hyaluronan: a possible pathophysiological mechanism. J Cutan Pathol 2005; 32: 612–615.
18. Fazeli A, Lio PA, Liu V. Nephrogenic fibrosing dermopathy: are ACE inhibitors the missing link? Arch Dermatol 2004; 140: 1401.
19. Cowper SE, Bucala R. Nephrogenic fibrosing dermopathy: suspect identified, motive unclear. Am J Dermatopathol 2003; 25: 358.
20. Ting WW, Stone MS, Madison KC, Kurtz K. Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol 2003; 139: 903–906.
21. Taylor RS, Levine JM, Jimenez SA. Case 35-2004: Nephrogenic fibrosing dermopathy. N Engl J Med 2005; 352: 1723–1724.
22. Ortonne N, Lipsker D, Chantrel F, Boehm N, Grosshans E, Cribier B. Presence of CD45RO+CD34+ cells with collagen synthesis activity in nephrogenic fibrosing dermopathy: a new pathogenic hypothesis. Br J Dermatol 2004; 150: 1028–1054.
23. Baron PW, Cantos K, Hillebrand DJ, Hu KQ, Ojogho ON, Nehlsen-Cannarella S, Concepcion W. Nephrogenic fibrosing dermopathy after liver transplantation successfully treated with plasmapheresis. Am J Dermatopathol 2003; 25: 204–209.
24. Chung HJ, Chung KY. Nephrogenic fibrosing dermopathy: response to high dose intravenous immunoglobulin. Br J Dermatol 2004; 150: 596–624.
25. LeBoit PE. What nephrogenic fibrosing dermopathy might be. Arch Dermatol 2003; 139: 928–930.
26. Kafi R, Fisher GJ, Quan T, Shao Y, Wang R, Voorhees JJ, Kang S. UV-A1 phototherapy improves nephrogenic fibrosing dermopathy. Arch Dermatol 2004, 140: 1322–1324.
27. Schmook T, Budde K, Ulrich C, Neumayer HH, Fritsche L, Stockfleth E. Successful treatment of nephrogenic fibrosing dermopathy in a kidney transplant recipient with photodynamic therapy. Nephrol Dial Transplant 2005; 20: 220–222.
28. Rose R, Lyon C. The successful treatment of nephrogenic fibrosing dermopathy with mycophenolate mofetil. J Am Acad Dermatol 2005; 52: 62.

