The aim of this validation study was to assess the measurement properties of the CECA (Spanish acronym for the Specific Questionnaire for Condylomata Acuminata) in patients with anogenital condylomas. A total of 247 patients aged > 18 years completed the questionnaire on 2 occasions as well as the Dermatology Life Quality Index (DLQI). The CECA questionnaire showed good internal consistency (Cronbach’s α values of 0.86 and 0.91 in the emotional and sexual activity dimensions) and good test-retest reliability (intraclass correlation coefficient 0.76 emotional dimension, 0.82 sexual activity dimension). Patients with de novo lesions and those with more extensive lesions and larger number of warts showed poorer health-related quality of life. CECA and DLQI scores correlated moderately. Patients whose lesions cleared at follow-up or with a reduction of ≥ 50% showed a better improvement of health-related quality of life. The CECA questionnaire is a valid, reliable and sensitive tool for the assessment of health-related quality of life in patients with anogenital warts. Key words: genital diseases, female; genital diseases, male; quality of life; questionnaires; papillomavirus infections; warts; psychology.
(Accepted November 12, 2007.)
Acta Derm Venereol 2008; 88: 257–262.
J. J. Vilata, Department of Dermatology, Consorcio Hospital General Universitario, Av. Tres Cruces 2, ES-46014 Valencia, Spain. E-mail: vilatacorell@eresmas.net
The prevalence of human papillomavirus (HPV) infection has risen steadily over the past 20 years worldwide, and it is estimated that 1% of the sexually active population is infected (1–3). Condylomata acuminata (also called genital warts or venereal warts), an epidermal manifestation attributed to HPV (4), in particular to HPV types 6 and 11, is one of the most common sexually transmitted diseases (5, 6). Genital warts are particularly frequent in young adults in the third decade of life and in older teenagers (7). Generally, two-thirds of individuals who have sexual contact with an infected partner develop lesions within 1–6 months (5).
Anogenital warts can cause psychological distress by making patients feel ashamed and less attractive, thereby reducing quality of life. It has been shown that a high level of anxiety, anger and depression is associated with the diagnosis and treatment of genital warts, and approximately two-thirds of patients had made lifestyle changes regarding sexual relationships (8). Sexual enjoyment and activity are also negatively affected (9). A better understanding among healthcare providers of the psychosexual aspects of the disease is pivotal to effective disease management and patient counselling (10).
The increasing interest in measures reflecting the personal viewpoint of patients’ health has led to an extended demand for reliable and valid standardized questionnaires of health-related quality of life (HRQL) (11). Disease-specific questionnaires, those that only contain items specifically designed for a particular condition, are more likely to be relevant and sensitive to patients in areas that clinicians may wish to monitor (12). In patients with genital condylomata acuminata, a specific HRQL questionnaire, called CECA (Cuestionario Específico para Condiloma Acuminado), has been developed with the objective of being used in clinical research and clinical practice. The development process of this instrument has been reported previously (13).
The objective of this validation study was to assess the measurement properties of the CECA questionnaire in patients of both sexes suffering from anogenital condylomata acuminata.
material and METHODS
From September 2004 to June 2005, 37 dermatologists, gynaecologists and physicians working in sexually transmitted disease clinics in 32 centres in Spain agreed to participate in a clinical observational research study. The purpose of the study was to assess the measurement properties of the CECA questionnaire in the routine clinical setting. Patients of both sexes ≥ 18 years of age with a clinical diagnosis of anogenital condylomata acuminata were eligible provided that they gave written informed consent and were able to understand and complete the study questionnaires. Immunosuppressed patients were excluded, as were those with any other skin disease involving the anogenital area that could interfere with the study. Participation in a clinical study in the previous 30 days was also an exclusion criterion. Each investigator enrolled approximately 10 patients. The study protocol was approved by the ethics committee of Hospital Clínic, Barcelona, Spain.
Patients who fulfilled the inclusion criteria were divided into 2 groups: (i) patients with de novo anogenital warts or recurrent lesions who were candidates to receive treatment (CECA sensitivity data-set); and (ii) patients with persistent condylomata acuminata, with or without visible lesions, currently untreated and being followed by their physicians, with no expected clinical change for the subsequent 15 days (CECA reliability data-set).
At baseline, data on sociodemographic characteristics (sex, age and education level); sexual behaviour; history of sexually transmitted disease; clinical variables including number of lesions, extension, de novo or recurrent lesions, number of recurrences and time elapsed since diagnosis; clinical assessment of general health status (rated as “very good”, “good”, “fairly good”, “neither good nor bad”, “fairly bad”, “bad”, “very bad”) and co-morbid conditions were collected for all patients. The prescribed medication was recorded in patients included in the sensitivity group. The CECA questionnaire and the Spanish validated version of the Dermatology Life Quality Index (DLQI) (12, 14) were administered at the same time each visit. During the follow-up visit, at 10 ± 3 weeks from baseline for patients in the sensitivity group, and at 15 days from baseline for patients in the reliability group, clinical characteristics were evaluated and the CECA and DLQI questionnaires were again administered, in addition to changes in a single item of self-perceived health status with reference to baseline.
The CECA is a valid and reliable self-administered questionnaire to measure HRQL in patients with anogenital warts (13). It comprises 10 items and 2 dimensions. The emotional dimension includes 6 items and the sexual activity dimension includes 4 items, as detailed in Table I. The questions refer to the past 7 days. The higher the score the better the quality of life. The global scoring range was 10–50, ranging from 6 to 30 in the emotional dimensions and from 4 to 20 in the sexual activity dimension. All dimensions were standardized for a scoring between 0 (worst HRQL) and 100 (best HRQL) in order to facilitate interpretation and comprehension. The questionnaire was designed to be self-administered.
Table I. Description of the CECA questionnaire
| Item |
| Emotional dimension |
| 1 | ”I am afraid that the lesions won’t disappear” |
| 2 | ”I am anxious to know whether I am going to recover from the infection for good” |
| 3 | ”I worry about whether the warts will get worse or if there will be some complications” |
| 4 | ”My state of mind is upset (anxiety, depression, sadness, uneasiness…)” |
| 5 | ”I feel more insecure” |
| 6 | ”Knowing that I have the illness affects me in my daily life” |
| Sexual dimension |
| 7 | ”My sexual drive has decreased” |
| 8 | ”I fell worried during the act” |
| 9 | ”I avoid sexual relations” |
| 10 | ”My sexual relations have decreased in quality and/or frequency |
Each question allows an answer on a 5-option Likert scale: ”always” = 1, ”almost always” = 2, ”sometimes” = 3, ”rarely” = 4, ”never” = 5 (items 1 and 3 also allowed the option of ”not applicable” scored as ”never” = 5).
CECA: Spanish acronym of Specific Questionnaire for Condylomata Acuminata.
The DLQI is a specific self-administered questionnaire for people with skin diseases. It contains 10 items and covers the domains of symptoms and feelings, daily activities, leisure, work and school, personal relationships and treatment. The answers are in a Likert scale, there being 4 categories (“very much”, “a lot”, “a little”, “not at all”). Scores range from 0 to 30. The higher the score, the more quality of life is impaired. The DLQI has been translated and validated for use in the Spanish population (12, 14).
The item on self-perceived health status is a single question about the change in the patient’s overall health status with reference to baseline. The item has 6 possible response options: “much better”, “better”, “slightly better”, “almost the same”, “slightly worse” and “worse”.
Statistical analysis
The required study sample size was calculated for each of the study groups. For the CECA sensitivity group, the sample size was calculated to be able to detect an effect size higher or equal to 0.2 in the CECA scores with a significance level of 0.05 and a statistical power of 0.80, for which a sample of 196 patients was necessary. For the CECA reliability group, the objective was to estimate the intraclass correlation coefficient (ICC), expected to be higher or equal to 0.7 with a minimum of 0.5, taking into account the same level of significance and statistical power, for which at least 63 patients were required.
A descriptive and comparative analysis of sociodemographic data, sexual behaviour and clinical characteristics of patients according to the study group was carried out using the χ2 test for the categorical variables and the Student’s t-test for the continuous variables. The feasibility of the CECA, defined as the percentage of patients who answered the questionnaire in full and the time needed to do it, was evaluated. The questionnaire’s reliability was analysed in terms of internal consistency and test-retest reliability. Internal consistency was evaluated in all patients using Cronbach’s α coefficient. Test-retest reliability was assessed by the ICC. Clinical stable patients were defined as patients in the reliability group with no clinical changes in their lesions and reporting health status as “almost the same” in the follow-up visit.
The construct validity of the questionnaire was assessed by the relationship between CECA scores and patient’s clinical variables. It may be expected that patients with a larger number of lesions, more extensive lesions, or who had had more relapses prior to the study, as well as patients in the sensitivity group, would show more impaired HRQL. The relationship between CECA and DLQI scores was assessed using Spearman’s correlation coefficient. Because the lowest score in CECA and the lowest score in DLQI represented the worst and the best HRQL, respectively, the expected correlation would be negative. The questionnaire’s validity over time was evaluated in the sensitivity group by comparing changes in CECA scores between baseline and follow-up regarding clearance of lesions or reduction of the affected area by ≥ 50%. Sensitivity to change was evaluated in the corresponding group of patients by analysing changes in the CECA scores regarding modifications in general health status observed by the patients themselves during the follow-up period. Effect size was calculated by dividing the difference between the mean score for the baseline visit and that of the follow-up visit by the standard deviation (SD) score for the baseline visit.
Double data entry was carried out with a subsequent validation to guarantee the quality and consistency of the data. A statistical significance level of p < 0.05 was used in all statistical tests performed. The statistical programme SPSS for Windows version 10.0 (SPSS, Inc., Chicago, Illinois, USA) was used to perform the entire data analysis.
RESULTS
Out of the 307 patients initially recruited, 231 for the sensitivity group and 76 for the reliability group, 60 were excluded, giving a final sample of 247. Forty-five patients withdrew from the sensitivity group (failure to attend follow-up visit at the planned interval 10 ± 3 weeks from baseline, n = 35; missed follow-up visit, n = 9; patient’s decision to discontinue the study, n = 1) and 15 from the reliability group (no longer stable lesion at the follow-up visit, n = 10; missed follow-up visit, n = 5). Therefore, the study population comprised 186 patients in the sensitivity group and 61 in the reliability group. Table II shows the sociodemographic characteristics, sexual behaviour and clinical data of the general population and the patient groups. There were no significant differences between patients in the sensitivity group and patients in the reliability group regarding male/female ratio, mean age, education level and sexual behaviour. However, the reliability group showed a significantly higher percentage of patients with prior diagnosis of condyloma acuminatum, longer time since diagnosis, lesser number of lesions, which in turn were less extensive than patients in the sensitivity group. All patients in the sensitivity group were treated for anogenital warts at the baseline visit, including 5% imiquimod cream in 51% of cases, cryotherapy in 26%, electrocoagulation in 7%, imiquimod cream and cryotherapy in 6% and other modalities in 10%.
Table II. Sociodemographic and clinical characteristics of patients with genital condylomata acuminata
| Data | Overall population n = 247 | Sensitivity group n = 186 | Reliability group n = 61 | p-value |
| Sex, n (%) | | | | 0.77 |
| Males | 132 (53.4) | 98 (52.7) | 34 (55.7) | |
| Females | 115 (46.6) | 88 (47.3) | 27 (44.3) | |
| Age, years, mean (SD) | 32.5 (9.3) | 32.1 (9.0) | 33.7 (10.3) | 0.28 |
| Level of education, n (%) | | | | 0.43 |
| Primary | 56 (22.7) | 42 (22.6) | 14 (23.0) | |
| Secondary | 115 (46.6) | 89 (47.8) | 26 (42.6) | |
| Higher | 60 (24.3) | 41 (22.0) | 19 (31.1) | |
| Unknown | 16 (6.5) | 14 (7.5) | 2 (3.3) | |
| Sexual behaviour, n (%) | | | | 0.11 |
| Heterosexual | 207 (83.8) | 159 (86.5) | 48 (78.7) | |
| Homosexual | 24 (9.7) | 18 (9.7) | 6 (9.8) | |
| Bisexual | 10 (4.0) | 7 (3.8) | 3 (4.9) | |
| Unknown | 6 (2.4) | 2 (1.1) | 4 (6.6) | |
| Prior diagnosis of sexually transmitted disease, n (%) | 52 (21.1) | 47 (28.4) | 5 (8.2) | < 0.01 |
| Prior diagnosis of condyloma acuminatum, n (%) | 129 (52.2) | 88 (47.3) | 41 (67.2) | < 0.01 |
| Time since diagnosis, days, mean (SD) | 301 (738) | 142 (300) | 781 (1280) | < 0.01 |
| Lesions | | | | |
| No lesions | 35 (14.2) | 0 | 35 (57.4) | < 0.01 |
| Number of lesions, mean (SD) | 6.2 (6.0) | 7.1 (5.9) | 3.3 (5.4) | < 0.01 |
| Size of lesions, mm2 | | | | |
| < 50 | 128 (51.8) | 106 (57.0) | 22 (36.1) | |
| 50–200 | 68 (27.5) | 64 (34.4) | 4 (6.6) | |
| > 200 | 16 (6.5) | 16 (8.6) | 0 | |
| Localization n (%) | | | | |
| Men | 110 | 98 | 12 | |
| Penis | 90 (81.8) | 79 (80.6) | 11 (91.7) | |
| Perianal region | 22 (20) | 21 (21.4) | 1 (8.3) | |
| Scrotum | 10 (9.1) | 9 (9.2) | 1 (8.3) | |
| Inguinal area | 8 (7.3) | 8 (7.3) | | |
| Other | 9 (8.2) | 7 (7.1) | 2 (16.7) | |
| Women | 102 | 88 | 14 | |
| Vulva | 84 (82.4) | 70 (79.5) | 14 (100) | |
| Perianal region | 36 (35.3) | 35 (39.8) | 1 (7.1) | |
| Perineal area | 34 (33.3) | 34 (33.3) | 0 | |
| Inguinal area | 1 (1.0) | 1 (1.1) | 0 | |
| Other | 11 (10.8) | 11 (12.5) | 0 | |
| Relapses, mean (SD) | 1.8 (1.0) | 1.8 (2.7) | 1.9 (1.0) | 0.45 |
| SD: standard deviation. | | | | |
The CECA was administered to 99.2% of the patients. The mean (SD) time to complete the questionnaire was 6.9 (6.1) min. The CECA questionnaire showed a good internal consistency, with Cronbach’s α values of 0.91 for the overall score and 0.86 and 0.91 for the emotional and sexual activity dimensions, respectively. The ICC between scores on the 2 administrations in the reliability group was 0.79, which was higher in the emotional dimension than in the sexual activity dimension (0.82 and 0.76, respectively).
The mean (SD) scores in the sensitivity group were significantly lower than in the reliability group with regard to overall CECA scores (40.5 (22.8) vs. 55.6 (22.7)), scores for the emotional dimension (37.0 (22.4) vs. 50.3 (24.7)) and scores for the sexual dimension (45.7 (29.0) vs. 64.5 (28.7)) (p < 0.01). As shown in Table III, global CECA scores and values for the emotional and sexual activity dimensions were significantly different according to the number and extension of lesions; that is, the fewer and smaller the lesions, the higher the scores and the better the quality of life. No statistically significant differences in CECA scores according to the number of recurrences were observed.
Table III. Differences in CECA scores in patients with condylomata acuminata according to number and size of lesions
| Data | CECA scores, mean (SD) |
| Overall | Emotional dimension | Sexual activity dimension |
| Number of lesions | | | |
| None | 56.0 (20.6) | 49.6 (22.7) | 67.1 (24.2) |
| 1 or 2 | 47.7 (26.5) | 43.8 (28.0) | 53.7 (30.3) |
| 3–5 | 42.7 (20.2) | 38.2 (20.5) | 49.2 (26.2) |
| 6–10 | 39.1 (23.6) | 37.8 (21.3) | 41.2 (33.7) |
| > 10 | 41.8 (27.5) | 37.2 (28.4) | 48.8 (30.7) |
| p-value | < 0.01 | < 0.01 | < 0.01 |
| Size of lesions, mm2 | | | |
| < 50 | 46.4 (23.3) | 42.1 /23.8) | 52.7 (29.3) |
| 50–200 | 37.2 (23.2) | 34.9 (22.7) | 40.8 (30.6) |
| > 200 | 31.3 (21.4) | 28.1 (19.9) | 35.9 (25.3) |
| p-value | < 0.01 | < 0.05 | < 0.01 |
CECA: Spanish acronym of Specific Questionnaire for Condylomata Acuminata; SD: standard deviation.
Correlation between CECA and DLQI scores ranged from moderate to high (Table IV). The emotional and personal relationships dimensions of the DLQI showed the highest correlations with the emotional dimension (r2 = –0.528) and the sexual activity dimension (r2 = –0.673) of the CECA as they measured the same HRQL aspects.
Table IV. Correlations between the CECA dimensions and the dermatology life quality index (DLQI) dimensions
| DLQI scores | CECA scores |
| Overall | Emotional dimension | Sexual activity dimension |
| Overall score | –0.670 | –0.546 | –0.676 |
| Symptoms and Feelings | –0.610 | –0.528 | –0.580 |
| Daily Activities | –0.505 | –0.414 | –0.504 |
| Leisure | –0.456 | –0.362 | –0.469 |
| Work and School | –0.408 | –0.332 | –0.411 |
| Personal relationships | –0.638 | –0.495 | –0.673 |
| Treatment | –0.425 | –0.369 | –0.404 |
Spearman’s correlation coefficient.
CECA: Spanish acronym of Specific Questionnaire for Condylomata Acuminata.
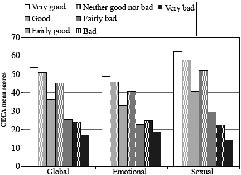
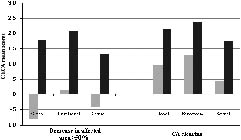
The relationship between mean scores of the CECA questionnaire and patients’ assessment of general health status at baseline is shown in Fig. 1. Patients who rated health status as very good or good had significantly higher CECA scores than the remaining categories, whereas those who rated health status as very bad, bad or fairly bad scored significantly lower in the CECA questionnaire. On the other hand, changes in CECA scores between baseline and follow-up indicating an improvement in HRQL were only observed amongst patients showing clearance of lesions or reduction of the affected area by ≥ 50% (Fig. 2).
Fig. 1. CECA questionnaire scores obtained from patients at the trial baseline visit, based on how the patients perceived their overall health status at the time. CECA: Spanish acronym of Specific Questionnaire for Condylomata Acuminata.
Fig. 2. Changes observed in CECA score according to clinical response. CECA: Spanish acronym of Specific Questionnaire for Condylomata Acuminata. No (), Yes(). CA: condyloma acuminata.
The effect size of the changes in the overall CECA scores and in emotional and sexual dimensions increased as the changes perceived by patients became more substantial: that is, the effect size was low when patients reported no change (“almost the same”) in their health status (–0.06 overall score, –0.16 emotional dimension, 0.12 sexual activity dimension), moderate when they reported feeling “slightly better” (–0.34 overall score, –0.48 emotional dimension, –0.03 sexual activity dimension) and large when patients reported feeling “much better” (–0.96 overall score, –1.09 emotional dimension, –0.61 sexual activity dimension). The effect size of the total sample reporting improvement in health status was higher for the CECA questionnaire than for the DLQI questionnaire (overall scores –0.78 and 0.51, respectively).
DISCUSSION
The results of the present study provide evidence that the CECA questionnaire, a disease-specific questionnaire for external anogenital warts, is feasible, valid, reliable and responsive to change for patients with condylomata acuminata and may be a useful assessment tool in the routine clinical setting and for research purposes. The CECA questionnaire contains only 10 items, it can be administered in 7 min, is highly acceptable to patients and simple to score. In terms of psychometric properties, the internal consistency of the CECA was high, with Cronbach’s α values of 0.91 for the overall score and 0.86 and 0.91 for the emotional and sexual activity dimensions, respectively. In the test-retest reliability, the ICC was also higher than the psychometric standard, with ICC values of 0.79 for the overall score and 0.82 and 0.76 for the emotional and sexual activity dimensions, respectively.
The discriminant capacity of the CECA is reflected by the differences obtained in the questionnaire scores amongst patient groups with different disease stages, i.e. de novo or recurrent lesions vs. persistent condylomata acuminata, reduced number of lesions vs. multiple lesions, small lesions vs. large lesions. However, the number of relapses prior to the study was not associated with higher impact on the quality of life. In fact, history of relapses does not constitute an indication of the current impact of the disease on the patient’s quality of life. It may be expected that patients with a higher number of recurrences would also have had a longer course of the disease and proportionally more time to develop coping behaviours. Moreover, it has been shown that the influence of HPV infection on a range of initial emotional reactions of anger, depression, isolation, shame and guilt decreased over time, and that there are multiple psychological and social factors other than disease issues that affect HRQL in patients with anogenital condylomata acuminata (8).
The CECA questionnaire has shown a moderate-to-high correlation with the DLQI questionnaire, correlation being higher for those dimensions that assessed similar aspects. The sensitivity to change of DLQI instrument was low and does not allow for an assessment of aspects more specific to anogenital warts. As expected, the effect size of the total sample reporting improvement in health status was higher for the CECA questionnaire than for the DLQI questionnaire.
The increasing number of generic and specific questionnaires developed during the last years to evaluate HRQL reflects their utility in the assessment of health outcomes. The use of HRQL instruments provides additional information to health professionals about patients’ health status, which is complementary to the clinical results measured by traditional outcomes. HRQL measurements facilitate communication between health professionals and patients and help health professionals to understand patients’ problems or health concerns and to evaluate the impact of a disease in patients’ lives.
In conclusion, this study shows that the CECA questionnaire is a valid tool for assessing HRQL in patients with anogenital condylomata acuminata. It is highly recommended for use in clinical research and daily practice due to its good psychometric properties and feasibility (it is easy to administer and effective).
ACKNOWLEDGEMENTS
The authors thank Marta Pulido, MD, for editing the manuscript and for editorial assistance.
ECAVIM Study Group: I. Puedo, Centro ETS, Sevilla; J. Ballesteros, Clínica Sandoval, Madrid; C. Colomo and A. Comunión, Centro ETS Montesa, Madrid; X. Camino, Hospital Donosita, San Sebastián-Donosti; M. T. Arguisjuela, Centro ETS, Sevilla; J. M. Rojo, Hospital de Valme, Sevilla; J. Ferrando and E. Barbera, CAP Baix Ebre, Tarragona; J. Boronat, Hospital Joan XXIII, Tarragona; P. Herranz, Hospital La Paz, Madrid; M. Sabán, CAP Ronda de Torrasa, Barcelona; A. Sevila, Hospital de San Juan, Alicante; B. Escutia, Hospital de Elda, Alicante; B. Numancia, Centro ETS Ayuntamiento, Zaragoza; M. García Font, Hospital Mútua de Terrassa, Barcelona; R. Ruiz, Hospital de Poniente, Almería; E. Herrera and A. Tejera, Hospital Clínico, Málaga; M. Velasco, Hospital Arnau de Vilanova, Valencia; E. Jordá, Hospital Clínico Universitario, Valencia; J. Xercavins and C. Centeno, Hospital Materno-infantil Vall d’Hebron, Barcelona; M. Quílez, Hospital de la Santa Creu i Sant Pau, Barcelona; M. Durán, Centro Especialidades M. Angeles Gómez, Madrid; J. A. Cortell, Hospital Nuestra Señora de la Candelaria, Tenerife; F. Blanco, Hospital de Mérida, Badajoz; P. Sánchez Valverde, Centro Atención Mujer Andraize, Pamplona; J. R. Rodríguez, Hospital Virgen de la Arrixaca, Murcia; L. M. Puig Tintoré and I. Alonso, Hospital Clínic i Provincial, Barcelona; O. Falcón, Hospital Materno Infantil, Las Palmas de Gran Canaria; and E. Peiry, Ambulatorio Numancia, Barcelona.
REFERENCES
1. Partridge JM, Koutsky LA. Genital human papillomavirus infection in men. Lancet Infect Dis 2006; 6: 21–31.
2. Shin HR, Franceschi S, Vaccarella S, Rih JW, Ju YH, Oh JK, et al. Prevalence and determinants of genital infection with papillomavirus, in female and male university students in Busan, South Korea. J Infect Dis 2004; 190: 468–476.
3. Nyári TA, Kalmár L, Deák J, Szollosi J, Farkas I, Kovacs L. Prevalence and risk factors of human papilloma virus infection in asymptomatic women in southeastern Hungary. Eur J Obstet Gynecol Reprod Biol 2004; 115: 99–100.
4. Auvinen E, Niemi M, Malm C, Zilliacus R, Trontti A, Fingerroos R, et al. High prevalence of HPV among female students in Finland. Scand J Infect Dis 2005; 37: 873–876.
5. Revzina NV, Diclemente RJ. Prevalence and incidence of human papillomavirus infection in women in the USA: a systematic review. Int J STD AIDS 2005; 16: 528–537.
6. Orduña Domingo A, Chu JJ, Eiros Bouza JM, Bratos Pérez MA, Gutiérrez Rodríguez MP, Almaraz Gómez A, et al. Distribución por edad y sexo de las enfermedades de transmisión sexual en Valladolid. Estudio de 5.076 casos. Rev Sanid Hig Publica (Madr) 1991; 65: 247–258.
7. Maw RD, Reitano M, Roy M. An international survey of patients with genital warts: perceptions regarding treatment and impact on lifestyle. Int J STD AIDS 1998; 9: 571–578.
8. Clarke P, Ebel C, Catotti DN, Stewart S. The psychosocial impact of human papillomavirus infection: implications for health care providers. Int J STD AIDS 1997; 7: 197–200.
9. Ireland JA, Reid M, Powell R, Petrie KJ. The role of illness perceptions: psychological distress and treatment-seeking delay in patients with genital warts. Int J STD AIDS 2005; 16: 667–670.
10. Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Intern Med 1993; 118: 622–629.
11. Patrick DL, Deyo RA. Generic and disease-specific measures in assessing health status and quality of life. Med Care 1989; 27: S217–232.
12. Badia X, Colombo JA, Lara N, Llorens MA, Olmos L, Sainz de los Terreros M, et al. Combination of qualitative and quantitative methods for developing a new Health Related Quality of Life measure for patients with anogenital warts. Health Qual Life Outcomes 2005; 3: 24, doi:10.1186/1477-7525-3-24.
13. De Tiedra AG, Nercadal J, Badia X, Mascaró JM, Herdman M, Lozano R, et al. Adaptación transcultural al español del Cuestionario Dermatology Life Quality Index (DLQI): el índice de Calidad de Vida en Dermatología. Actas Dermo-Sifilogr 1998; 89: 692–700.
14. Badia X, Mascaró JM, Lozano R on behalf of the Cavide Research Group. Measuring health-related quality of life in patients with mild to moderate eczema and psoriasis: clinical validity, reliability and sensitivity to change of DLQI. Br J Dermatol 1999; 141: 698–702.