Polymorphic light eruption (PLE), with an overall prevalence of 10–20%, is mainly provoked by ultraviolet A (UVA) (320–400 nm) and to a lesser degree by UVB (280–320 nm). The most effective prophylaxis of PLE, application of UV protection clothing, is not feasible for all sun-exposed areas of the skin and UV-hardening is time-consuming and may be associated with side-effects. Most sunscreens protect predominantly against UVB and therefore fail to prevent PLE. The protection level of potent UVA-protective filters remains unresolved. This single-centre, open, placebo-controlled, intra-individual, comparative study, analysed the efficacy of a sunscreen of very high protection level against UVB and UVA, containing methylene bis-benzotriazolyl tetramethylbutylphenol (Tinosorb M), bis-ethylhexyloxyphenol methoxyphenyl triazine (Tinosorb S) and butyl methoxydibenzoylmethane as UVA absorbing filters, in the prevention of PLE under standardized photodiagnostic conditions. After determination of the minimal erythema dose at day 0, photoprovocation was performed in 12 patients with a clinical history of PLE, on days 1, 2 and 3 with 100 J/cm2 UVA and variable doses of UVB, starting with the 1.5-fold minimal erythema dose of UVB. Prior to irradiation, placebo was applied to the right and sunscreen to the left dorsal forearm under COLIPA (European Cosmetic, Toiletry and Perfumery Association) conditions. In 10 patients PLE could be provoked at the placebo site, with positive reactions in 90% of the UVA, 40% of the UVB and 90% of the UVA/UVB irradiated fields. At the site with the active treatment none of these patients developed PLE. These data demonstrate that a sunscreen with effective filters against UVA and UVB can successfully prevent the development of PLE. Further studies are needed to examine whether regular application of sunscreen under everyday conditions, especially in doses less than the tested COLIPA-norm, could be an equivalent alternative to UV-hardening therapy. Key words: sunscreen; polymorphic light eruption; photoprotection; UVA.
(Accepted April 10, 2008.)
Acta Derm Venereol 2008; 88: 555–560.
Mark Berneburg, Department of Dermatology, University of Tübingen, Liebermeisterstr. 25, DE-72076 Tübingen, Germany. E-mail: mark.berneburg@med.uni-tuebingen.de
Polymorphic light eruption (PLE) is one of the most frequent sun-induced skin diseases, with a prevalence of up to 20% of the population reported in the literature (1–3). It frequently develops in young adulthood and persists for most of the patient’s life (4). PLE is characterized by itching or painful erythema, papules, nodules, vesicles or bullae, localized predominantly on sun-exposed areas of the body, especially the face, hands, forearms and cleavage (5). PLE occurs mainly in spring or early summer, but in affected individuals it can persist throughout the summer (6). Most of the time, PLE improves during the summer (7), but when sun exposure is too strong, this mechanism may be insufficient (8). The most effective prophylaxis of PLE is the application of ultraviolet (UV) protective clothing, but this is not suitable for areas such as the face or hands (9, 10). Experience with “natural light” hardening has therefore led to the introduction of various UV-therapies in the prevention of PLE, with UVA (11, 12), UVB (13–15), UVB 311 nm (16, 17) or photochemotherapy (psoralen and UVA treatment; PUVA) (13, 14, 16–18). More severe cases have to be treated with glucocorticoids (5, 19) or stronger immunosuppressive agents (20, 21). The disadvantages of these treatment modalities are time-intensiveness or side-effects caused by the different treatment modalities.
Previous studies have shown that PLE is provoked mainly by UVA (320–400 nm) and, to a lesser extent, by UVB (280–320 nm), indicating a role for oxidative stress in the pathogenesis of PLE (18, 22–24). As the majority of sunscreens protect mainly from UVB, but fail to protect from UVA, they cannot sufficiently prevent patients from developing PLE (8, 25). Insufficient development of sunscreens against UVA is due to the fact that the wavelength of UVA irradiation is very close to that of visible light. Therefore, it is very difficult to develop cosmetically acceptable sunscreens without leaving a white film on the skin, leading to an unsatisfactory compliance level. Another problem is potential photosensitization in the case of chemical UVA-filters. Thus, many sunscreens are not useful in the prevention of PLE and may even aggravate the disease.
We have shown previously that UVA-blocking sunscreens protect users effectively from the development of lupus erythematosus (LE) (26). Approximately 8–12% of patients with PLE are positive for antinuclear antibodies (27, 28), and clinical symptoms of PLE seem to be common in patients with both systemic and cutaneous LE (29–31). It has been suggested that in approximately half of the patients with LE, PLE may precede LE (29) or that cutaneous manifestation of LE may present as PLE (27). This close relationship suggests that a UV-blocking sunscreen may also protect users from the development of PLE. UVA filtering compounds such as alpha-glycosylrutin (AGR), alone or in combination with antioxidants, have been shown to protect from development of PLE, but sun protection did not exceed a sun protection factor (SPF) of 15 and protection from PLE never reached 100% (32–34).
The current single-centre, open, placebo-controlled, intra-individual, comparative study tested a sunscreen that has already shown highly effective filtering against UVA irradiation in physical tests and been proven not to cause sensitization or photoallergy in in vivo tests in humans. The aim of this study was to examine the efficacy of this sunscreen of very high protection level containing the UVA absorbing filters methylene bis-benzotriazolyl tetramethylbutylphenol (Tinosorb M), bis-ethylhexyloxyphenol methoxyphenyl triazine (Tinosorb S) and butyl methoxydibenzoylmethane in the prevention of PLE during a diagnostic photoprovocation test under standardized photodiagnostic conditions. Patients with a clinical history of PLE who were scheduled to undergo photoprovocation for diagnosis were recruited to the study. In parallel with this PLE provocation test, the efficacy of this UVA-filter in the prevention of PLE was analysed by comparing sunscreen with vehicle.
MATERIALS AND METHODS
The study was approved by the local ethics committee (number 456.2004) as well as the national government authority for medical compounds (BfArM number 4030484, Eudra-CT number 2005-001346-18).
Patients
Twelve patients with a clinical history of PLE, who were scheduled to have a diagnostic photoprovocation test, were recruited after giving their written informed consent (intent to treat, ITT). They were numbered in chronological order, starting with 01. Two patients (numbers 8 and 10) were rated as drop-outs, as PLE could not be provoked during testing at the placebo site. The mean age of the remaining 10 patients (per protocol, PP) was 46.3 ± 5.2 years, 7 women and 3 men (numbers 1, 4 and 12). Inclusion and exclusion criteria are shown in Table I.
Table I. Inclusion and exclusion criteria
| Inclusion criteria | Exclusion criteria |
| • Clinical history of PLE • Duration of PLE for at least one summer season • 18 ≤ Age (years) ≥ 70 • Written informed consent | • Systemic application of antihistamines, corticosteroids, retinoids, hydroxychloroquine, immunosuppressive agents (e.g. methotrexate, cyclosporine), cytostatics or photosensiziting agents: psoralen, phenothiazine, tetracycline, chinolone, nalidixine acid, non-steroidal anti-inflammatory drugs, furosemide, fibrates, amiodarone phytopharmaca during or less than 4 weeks prior to study • Malignancies • Severe systemic diseases or infections prior to study • Psychiatric diseases or epilepsy • UV-therapy within the last 3 months prior to study • Pregnancy or breast-feeding • Known allergy or hypersensitivity regarding study medication • Dementia or mental state that does not allow perception of the therapy and therefore written consent. • Concomitant participation in another clinical trial or participation in another clinical trial within the last 14 days prior to randomization |
PLE: polymorphic light eruption; UV: ultraviolet.
Sunscreen
The applied sunscreen, Daylong®, has a “very high protection level” according the the manufacturer (Spirig Pharma Ltd, Egerkingen, Switzerland) and is widely available. The listed ingredients are: aqua, isoamyl p-methoxycinnamate, ethylhexyl methoxycinnamate, bisethylhexyloxyphenol methoxyphenyl triazine (Tinosorb S), ethylhexyl triazone, dicaprylyl maleate, methylene bisbenzotriazolyl tetramethylbutylphenol (Tinosorb M), butyl methoxydibenzoylmethane, alcohol, sorbitol, cetyl phosphate,tiethanolamine, tocopherol, aloe barbadensis, carbomer, cetyl alcohol, dimethicone, lecithin, decyl glucoside, propylene glycol, xanthan gum, methylparaben, propylparaben, sodium benzoate, citric acid, potassium sorbate and BHT.
In this study the sunscreen was compared with its vehicle without the following active substances: isoamyl pmMethoxycinnamate, ethylhexyl methoxycinnamate, bis-ethylhexyloxyphenol methoxyphenyl triazine (Tinosorb S), ethylhexyl triazone, methylene bis-benzotriazolyl tetramethylbutylphenol (Tinosorb M) and butyl methoxydibenzoylmethane.
Phototesting and evaluation procedures under standardized photodiagnostic conditions
The study was designed as a single-centre, open, placebo-controlled, intra-individual study, as described by Salomon et al. (3). This study design leads, in 74% of patients with a typical history of PLE, to the production of PLE-characteristic skin changes in our irradiation fields at 36 cm2 at the forearm as typical localizations. This photoprovocation test not only helps to diagnose PLE by controlled reproduction, but also determines which wavelengths lead to the development of the disease and proves the efficacy of sunscreens in the prevention of PLE.
In this study we determined the minimal erythema dose (MED) of UVB on day 0 as a marker for the sensitivity against UVB-irradiation (reading after 24 h). In addition, we determined immediate pigment darkening (IPD; immediate reading) and delayed pigment darkening (DPD; reading after 24 h). Both tests to estimate the sensitivity against UVA-irradiation were performed on non-sun-exposed gluteal skin.
Photoprovocation test under standardized photodiagnostic conditions
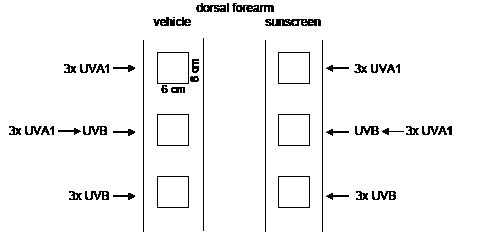
For photoprovocation on three consecutive days (day 1–3), three fields (field size 6 × 6 cm) next to each other on both dorsal forearms were irradiated as follows: (i) one field with 100 J/cm2 UVA 1; (ii) one field with 100 J/cm2 UVA 1 plus 1.5-fold MED UVB; and (iii) one field with 1.5-fold MED UVB (Fig. 1). If 1.5-fold MED UVB on gluteal skin did not cause erythema at the test site within 24 h, the UVB dose was increased on days 2 and 3. On the left dorsal forearm sunscreen was applied 30 min prior to irradiation in quantities of 2 mg/cm2, according to the recommendations of the US Food and Drug Administration and the European Cosmetic Toiletry and Perfumery Association (COLIPA norm). On the contralateral right dorsal forearm the vehicle, as placebo-control, was applied in the same manner. Readings were performed in each of the six fields every day prior to irradiation, immediately after irradiation, and 24 h after the last irradiation.
Fig. 1. Schematic diagram of test procedure. Both forearms were included in photodiagnostic procedures. One set of test fields, with an area of 6 × 6 cm, was treated with sunscreen (right panel), while the other set was equally treated with the vehicle control (left panel). Each set consisted of one field treated three times with UVA1 alone (top), three times with UVB alone (bottom) and three times UVA1 followed by UVB (middle). The order of the three fields varied from patient to patient.
Determination of MED, IPD, DPD were performed gluteally with the Saalmann Multitester SBB LT 400 (Saalmann, Herfordt, Germany). For photoprovocation, the Waldmann UV 800 lamp (for UVB, wavelength 280–320 nm) (Waldmann, Villingen-Schwenningen, Germany) and the Sellamed 4000 lamp (for UVA 1, wavelength 340–400 nm) (Sellas Medizingeräte, Gevelsberg, Germany) were used. The UV intensity of the lamps was controlled with the Waldmann UV-meter Variocontrol (Waldmann).
Evaluation
Evaluation was carried out according to the following graduation:
I. DPD/IPD: 0 = no pigmentation, P+ = slightly visible, sharply defined pigmentation, P++ = moderate pigmentation, P+++ = strong pigmentation.
II. MED: 0 = no erythema, E+ = slightly visible, sharply edged erythema, E++ = strong erythema, E+++ = very strong erythema with infiltration.
III. Skin reaction: 0 = no reaction, 1 = diffuse persistent erythema, 2 = sharply edged, persistent erythema, 3 = discrete infiltration 4 = strongly infiltrated papules and plaques, 5 = vesicles and bullae.
IV. Subjective sensation: no sensation, itching, burning, pain.
The skin reaction (III) was crucial to the decision as to whether PLE could be induced. Diffuse erythema without itching was not sufficient to diagnose PLE. Criteria for a positive reaction (PLE) were either diffuse persistent erythema concomitant with itching or a skin reaction ≥ 2.
Statistical analysis
Assuming a drop-out rate of 33%, 30 patients were planned to be included in the study (ITT). With a sample size of 20 valuable patients (PP) and an assumed efficacy of the sunscreen of 75% the exact 95% confidence interval for effecay would extend from 51 to 91%. After an intermediate analysis of the results the study could be finished already after 12 pateints (ITT). Statistical analysis was performed according to the exact sign test and exact confidence intervals for the efficacy were calculated. Levels were considered to be significant with p < 0.05.
RESULTS
Phototests
Two patients (numbers 8 and 10) were rated as drop-outs, as PLE could not be provoked at the placebo site during testing. In the 10 remaining patients PLE was provoked as per protocol by photoprovocation. These patients showed an MED UVB between 0.058 and 0.116 J/cm2. The IPD was between 20 and greater than 100 J/cm2, and the DPD between 40 and greater than 100 J/cm2 (Table II).
Table II. Results of photoprovocation in 10 patients with positive test results
| Patient number | PLE UVA | PLE UVB | PLE UVA/UVB | MED UVB (J/cm2) | IPD (J/cm2) | DPD (J/cm2) |
| 1 | Itching, papules | – | Itching, diffuse erythema | 0.099* | 60 | 60 |
| 2 | – | – | Itching, diffuse erythema | 0.099* | 20 | > 100 |
| 3 | Infiltrated erythema, papules | Papules | Papules | 0.088* | 40 | 40 |
| 4 | Itching, persistent erythema | – | Itching, infiltrated erythema | 0.088* | > 100 | > 100 |
| 5 | Itching, persistent erythema | Itching, diffuse erythema | Itching, persistent erythema | 0.099 | > 100 | > 100 |
| 6 | Itching, papules | Itching, papules | Itching, papules | 0.074* | 20 | 60 |
| 7 | Itching, infiltrated erythema, papules | – | Itching, infiltrated erythema, papules | 0.116 | > 100 | > 100 |
| 9 | Itching, papules | – | – | 0.074* | > 100 | > 100 |
| 11 | Itching, papules | – | Itching, papules | 0.116 | 40 | 40 |
| 12 | Papules | Papules | Itching, papules | 0.058* | 40 | 40 |
*In these patients the UVB dose used for irradiation had to be increased during photoprovocation above the 1.5-fold MED UVB.
PLE: polymorphic light eruption; MED: minimal erythema dose; IPD: immediate pigment darkening; DPD: delayed pigment darkening; UV: ultraviolet.
Photoprovocation
In 7 patients the UVB dose had to be increased after the first day of provocation due to missing erythema at the UVB-irradiated placebo fields. All patients then showed erythema and pigmentation in the fields irradiated with UVA, UVB and UVA/UVB in combination at the placebo arm (vehicle). PLE could be provoked in 9/10 patients (90%) by UVA, in 4/10 patients (40%) by UVB and in 9/10 patients (90%) by UVA/UVB. One patient developed PLE only in the UVA field, one patient only in the UVA/UVB combination field, four patients in two fields (UVA and UVA/UVB) (Figs 2 and 3) and four patients in all three irradiation fields UVA, UVB and UVA/UVB (Table II). PLE in the UVA field was characterized, in addition to variable diffuse or persistent erythema and pigmentation, by infiltrated erythema (20%), subjective sensations such as itching (70%) and development of papules (80%). In the UVB field symptoms comprised, also in addition to variable erythema and pigmentation, itching and papules (30% each). In the UVA/UVB combination field PLE manifested itself with infiltrated erythema (30%), itching (80%) and papules (50%) in addition to variable erythema and pigmentation (Table II).
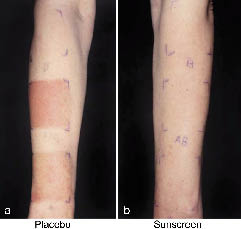
Fig. 2. Photoprovocation test in two-sided comparison. (a) Patient number 7 with polymorphic light eruption at day 5, showing a positive reaction to ultraviolet A (UVA) and UVA/UVB after photoprovocation, but no reaction to UVB alone. (b) No reaction to UVA/UBV was observed in the area to which sunscreen was applied. (NB: Marking for UVA alone is missing).
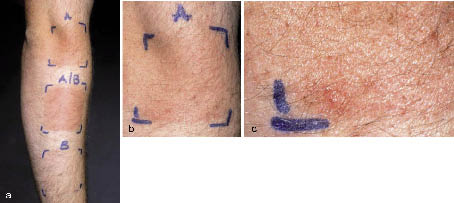
Fig. 3. Provocation of polymorphic light eruption (PLE) with UVA and UVA/UVB. (a) Patient number 1 with PLE after photoprovocation with UVA and UVA/UVB at day 5. (b, c) Showing itching, persistent erythema and papules.
At the arm treated with 2 mg/cm2 sunscreen 30 min prior to irradiation all 10 patients (100%) developing PLE on the control arm, were fully protected against PLE under standardized conditions.
According to the exact sign test 10 successes out of ten patients yields a p-value of 0.002. The 95% confidence interval for the efficacy of treatment is from 69 to 100%.
DISCUSSION
These data demonstrate with 95% confidence that the efficacy of the UVB- and UVA-protecting sunscreen in the prevention of PLE is at least 69%. We were able to induce PLE under standardized photodiagnostic conditions in 10 of 12 patients who presented with a history of PLE. In this population MED, IPD and DPD did not show clinically pathological readings.
PLE reactions could be observed in all of the UVA- or the UVA/UVB exposed fields in our study. This is consistent with the literature, where PLE is induced mostly by UVA. Four patients did show PLE reactions in the UVB field, but these patients also showed reactions in either UVA alone or in the UVA/UVB combination field.
PLE causes variable degrees of morbidity. Highly affected individuals suffer severe, as the disease is usually characterized by strong itching, burning or pain in addition to erythema, infiltration, papules or vesicles that normally persist for one or 2 days. In our study, reactions included itching, infiltrated and persistent erythema and papules that did not persist longer than 7 days, and patients described considerable distress due to these symptoms. Reactions were absent in test sites treated with sunscreen and patients did consider careful outdoor activities with short periods of ambient UV-exposure under these conditions.
For PLE, previous studies could show protection from solicitation of PLE lesions by AGR (32–34). These studies were either carried out in the presence or absence of antioxidants. While these studies suggest a role of oxidative stress in the pathogenesis of PLE, the compound used only provided a SPF of 15 and protection from the development of PLE lesions was never complete. The data from the current study show that regular application of the sunscreen tested, which has very high protection levels in both the UVB and the UVA range, is able to prevent development of PLE lesions in all individuals showing positive PLE photoprovocation in the placebo control arm. Since the compound used in our study did not reveal any photosensitizing potential, it can be considered to be safe as well as highly effective in the prevention of PLE caused by UVA and UVB irradiation. Further studies are needed to confirm this highly effective prevention of PLE when applied under daily conditions of sun-exposure.
Conflict of interest: This study was financed by a grant from Spirig Pharma Ltd, Egerkingen, Switzerland.
References
1. Holzle E, Plewig G, Hofmann C, Roser-Maass E. Polymorphous light eruption. Experimental reproduction of skin lesions. J Am Acad Dermatol 1982; 7: 111–125
2. Hawk JLM, Norris PG. Abnormal responses to ultraviolet radiation: idiopathic. In: Freedberg IM, Eisen AZ, Katz SI, Wolff K, Goldsmith LA, Austen KF, et al. Fitzpatricks´s dermatology in general medicine, 5th edn. New York: McGraw-Hill, 1999: p. 1573–1589.
3. Salomon N, Messer G, Dick D, Plewig G, Röcken M. Phototesting for polymorphic light eruption (PLE) with consecutive UVA1/UVB-irradiation. Photodermatol Photoimmunol Photomed 1997; 13: 72–74.
4. Jansen CT. The natural history of polymorphous light eruptions. Arch Dermatol 1979; 115: 165–169.
5. Tutrone WD, Spann CT, Scheinfeld N, Deleo VA. Polymorphic light eruption. Dermatol Ther 2003; 16: 28–39.
6. Pao C, Norris PG, Corbett M, Hawk JLM. Polymorphic light eruption: prevalence in Australia and England. Br J Dermatol 1994; 130: 62–64.
7. Hönigsmann H. Polymorphous light eruption. In: Lim HW, Soter NA, editors. Clinical Photomedicine. New York: Marcel Dekker, 1993: p. 167–180.
8. Ling TC, Gibbs NK, Rhodes LE. Treatment of polymorphic light eruption. Photodermatol Photoimmunol Photomed 2003; 19: 217–227.
9. Robson J, Diffey BL. Textiles and sun protection. Photodermatol Photoimmunol Photomed 1990; 7: 32–34.
10. Gies HP, Roy CR, Elliot G, Zongli W. Ultraviolet radiation protection factors for clothing. Health Phys 1994; 67: 131–139.
11. Rücker BU, Häberle M, Koch HU, Bocionek P, Schriever KH, Hornstein OP. Ultraviolet light hardening in polymorphous light eruption: a controlled study comparing different emission spectra. Photodermatol Photoimmunol Photomed 1991; 8: 73–78.
12. Berg M, Ros AM, Berne B. Utraviolet A phototherapy and trimethylpsoralen UVA photochemotherapy in polymorphous light eruption – a controlled study. Photodermatol Photoimmunol Photomed 1994; 10: 139–143.
13. Addo HA, Sharma SC. UVB phototherapy and photochemotherapy (PUVA) in the treatment of polymorphic light eruption and solar urticaria. Br J Dermatol 1987; 116: 539–547.
14. Murphy GM, Logan RA, Lovell CR, Morris RW, Hawk JLM, Magnus IA. Prophylactic PUVA and UVB therapy in polymorphic light eruption – a controlled trial. Br J Dermatol 1987; 116: 531–538.
15. Boonstra J, van Weelden H, Toonstra J, van Vloten WA. Polymorphous light eruption: a clinical, photobiologic, and follow-up study of 110 patients. J Am Acad Dermatol 2000; 42: 199–207.
16. Bilsland D, George SA, Gibbs NK, Aitchison T, Johnson BE, Gerguson J. A comparison of narrow band phototherapy (TL-01) and photochemotherapy (PUVA) in the management of polymorphic light eruption. Br J Dermatol 1993; 129: 708–712.
17. Man I, Dawe S, Ferguson J. Artificial hardening for polymorphic light eruption: practical points from ten years experience. Photodermatol Photoimmunol Photomed 1999; 15: 96–99.
18. Dummer R, Ivanova K, Scheidegger EP, Burg G. Clinical and therapeutic aspects of polymorphous light eruption. Dermatology 2003; 207: 93–95.
19. Patel DC, Bellaney GJ, Seed PT, McGregor JM, Hawk JL. Efficacy of short-course oral prednisolone in polymorphic light eruption: a randomized controlled trial. Br J Dermatol 2000; 143: 828–831.
20. Norris PG, Hawk JL. Successful treatment of severe polymorphous light eruption with azathioprine. Arch Dermatol 1989; 125: 1377–1379.
21. Shipley DRV, Hewitt JB. Polymorphic light eruption treated with cyclosporin. Br J Dermatol 2001; 144: 446–447.
22. Holzle E. PLD – Klinisches Bild und bisheriger Stand des Wissens zur Pathogenese, Prophylaxe und Therapie. Dt Derm 1997; 7: 679–680.
23. Lehmann P. Photodiagnostische Testverfahren in: Krutmann J, Hönigsmann H. (Hrsg). Handbuch der dermatologischen Phototherapie und Photodiagnostik. Berlin, Heidelberg: Springer, 1997: 313–324.
24. Mastalier U, Kerl H, Wolf P. Clinical, laboratory, phototest and phototherapy findings in polymorphic light eruptions: a retrospective study of 133 patients. Eur J Dermatol 1998; 8: 554–559.
25. Stege H, Budde M, Grether-Beck S, Richard A, Rougier A, Ruzicka T, Krutmann J. Sunscreens with high SPF values are not equivalent in protection form UVA induced polymorphous light eruption. Eur J Dermatol 2002; 12: IV–VI.
26. Herzinger T, Plewig G, Röcken M. Use of sunscreens to protect against ultraviolet-induced lupus erythematosus. Arthritis Rheum 2004; 9: 3045–3048.
27. Murphy GM, Hawk JLM. The prevalence of antinuclear antibodies in patients with apparent polymorphic light eruption. Br J Dermatol 1991; 125: 448–451.
28. Millard TP, Lewis CM, Khamashta MA, Hughes GRV, Hawk JLM, McGregor JM. Familial clustering of polymorphic light eruption in relatives of patients with lupus erythematosus: evidence of a shared pathogenesis. Br J Dermatol 2001; 144: 334–338.
29. Petzelbauer P, Binder M, Nikolakis P, Ortel B, Hönigsmann H. Severe sun sensitivity and the presence of antinuclear antibodies in patients with polymorphous light eruption-like lesions. J Am Acad Dermatol 1992; 26: 68–74.
30. Nyberg F, Hasan T, Puska P, Stephansson E, Hakkinen M, Ranki A, et al. Occurrence of polymorphous light eruption in lupus erythematosus. Br J Dermatol 1987; 116: 531–538.
31. Wechsler HL. Cutaneous disease in systemic lupus erythematosus. Clin Dermatol 1985; 3: 79–87.
32. Rippke F, Wendt G, Bohnsack K, Dorschner A, Stab F, Holzle E, et al. Results of photoprovocation and field studies on the efficacy of a novel topically applied antioxidant in polymorphous light eruption. J Dermatol Treat 2001; 12: 3–8.
33. Hadshiew IM, Treder-Conrad C, v Bülow R, Klette E, Mann T, Stab F, et al. Polymorphous light eruption (PLE) and a new potent antioxidant and UVA-protective formulation as prophylaxis. Photodermatol Photoimmunol Photomed 2004; 20: 200–204.
34. Jeanmougin M, Peyron JL, Thomas P, Beani JC, Guez E, Bachot N. Polymorphic light eruption: prophylaxis using a topical combination of antioxidants and UVA protection formulations. Ann Dermatol Venereol 2006; 133: 425–428.