Previous reports demonstrated an association between psoriasis and the metabolic syndrome. The aim of this study was to elucidate the association between psoriasis and dyslipidaemia. A cross-sectional study was performed utilizing a population-based database. Psoriasis patients were compared with enrollees without psoriasis regarding the prevalence of dyslipidaemia and lipid levels. Comparison of lipid levels was performed on a “low-risk” subset of subjects without diabetes, hypertension and cardiovascular disease. The study included 10,669 psoriasis patients and 22,996 subjects without psoriasis. The prevalence of dyslipidaemia was significantly higher in psoriasis patients (odds ratio (OR) = 1.48, 95% confidence interval (CI) 1.40–1.55). The association remained significant after controlling for confounders (OR = 1.19, 95% CI 1.12–1.26, p < 0.001). In multivariate analysis of the “low-risk” subset, triglyceride levels were higher in psoriasis patients and high-density lipoprotein cholesterol levels were lower. This study supports previous reports of an association between psoriasis and lipid abnormalities. Key words: dyslipidaemia; hyperlipidaemia; psoriasis; lipid levels; cholesterol; triglycerides; metabolic syndrome.
(Accepted April 21, 2008.)
Acta Derm Venereol 2008; 88: 561–565.
Jacob Dreiher, Siaal Research Center for Family Medicine and Primary Care, Faculty of Health Sciences, Ben-Gurion University of the Negev, PO Box 653, Beer-Sheva, 84150 Israel. E-mail: jacod@bgu.ac.il
Psoriasis is a chronic disorder characterized by erythematous scaly patches that affect the scalp, trunk, extensor surfaces of the limbs and the genital area. Psoriasis is highly prevalent in the general population, mainly as a result of its chronic nature and the absence of a cure. Psoriasis affects about 2–4% of the general population (1, 2). In Israel, the prevalence of psoriasis is estimated at 2% (Israel Society for Dermatology and Venereology, Personal Communication). The aetiology of psoriasis is unknown, but genetic, metabolic and immune mechanisms have been proposed (3). Psoriasis is associated with decreased quality of life and high rates of depression. Patients with mild to moderate psoriasis are usually given topical treatments. Systemic therapy or phototherapy is reserved for patients with moderate to severe psoriasis (1).
Most healthcare providers do not associate psoriasis with an unfavourable cardiovascular risk profile, but mounting evidence shows that this might be the case (4). Psoriasis is associated with markers of systemic inflammation, such as increased C-reactive protein. An elevated risk for other disorders associated with an inflammatory state has been described (5). Psoriasis has been associated with a high frequency of cardiovascular events, which seems to be related to the severity and duration of psoriasis (5–7). Several reports have demonstrated an increased risk for traditional cardiovascular risk factors, such as smoking, low physical activity, hypertension, obesity, diabetes mellitus and the metabolic syndrome (a combination of central obesity, diabetes mellitus type 2 or insulin-resistance, hypertension and combined dyslipidaemia) in patients with psoriasis (4–5, 7–16).
Various disorders of plasma lipid and lipoprotein pattern (3, 6, 11, 16, 17–20), most often including an increase in triglycerides and a decrease in high-density lipoprotein (HDL) cholesterol, have been shown (3, 4, 20). In some studies, significant increases in total cholesterol and low-density lipoprotein (LDL) cholesterol have also been found (3, 6, 18). Some medications used to treat psoriasis, such as oral retinoids and cyclosporine, may induce dyslipidaemia in some patients (13, 21). However, their use in Israel is currently low: 3.5% of psoriasis patients are treated with acitretin and 0.3% with cyclosporine (Clalit Health Services (CHS), unpublished data).
In previous studies we have described the association between psoriasis and ischaemic heart disease (22) and diabetes (15, 23). The purpose of the current study was to assess the association between psoriasis and dyslipidaemia utilizing the large medical dataset of CHS.
METHODS
For the current study, which was a retrospective cross-sectional study, data-mining techniques utilizing the CHS database were used. CHS is the largest health provider organization in Israel, serving a population of approximately 3,800,000 enrollees. A comprehensive computerized database with continuous real-time input from pharmaceutical, medical and administrative computerized operating systems facilitates epidemiological studies such as the current analysis.
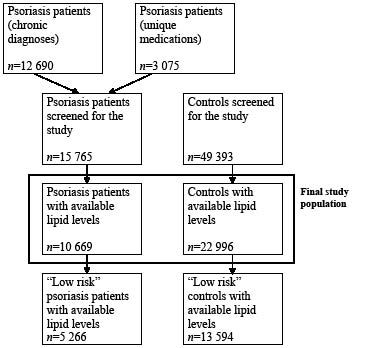
Patients were defined as having psoriasis when there was at least one documented diagnosis of psoriasis in the medical records registered by a CHS physician (in a primary care clinic or during hospitalization). Additional patients with psoriasis were added by identifying patients who use medications that are explicitly prescribed in Israel to patients with psoriasis (acitretin and calcipotriol) or use of psoralen with ultraviolet A (PUVA). A total of 12,690 psoriasis patients (80%) were identified based on a psoriasis diagnosis, and 3075 (20%) were identified through the use of specific drugs (acitretin, calcipotriol or PUVA). No data regarding specific treatments or confirmation of the diagnosis by a dermatologist was available. The control group was selected randomly from the list of CHS enrollees, excluding patients with a diagnosis of psoriasis. Data available from CHS database included age, gender, ethnicity (Jewish or Arab), geographic area of residence within Israel, chronic diagnoses, such as diabetes, hypertension, obesity, current smoking, ischaemic heart disease, cerebrovascular disease, and dyslipidaemia, as well as a large variety of diagnoses (109 different codes for chronic disease). The diagnoses of chronic diseases, including dyslipidaemia, were taken from the CHS chronic diseases registry, which is based on utilization of medications and data withdrawn from hospital and primary care physicians’ reports. A dyslipidaemia code is registered in the database when a diagnosis of dyslipidaemia is made by a primary care physician or during hospitalization, when patients are prescribed statins or fibrates, or when total cholesterol levels exceed 250 mg/dl. The registry is validated by primary physician confirmation of registered diagnoses of chronic diseases. The validity of diagnoses in the register was previously estimated and found to be high for important chronic diagnoses (24–25).
Current lipid levels, including total cholesterol, LDL cholesterol, HDL cholesterol and triglycerides, were available for 33,665 patients over the age of 20 years, out of 65,158 patients screened for the study, who were included in the present study (Fig. 1). Lipid levels were standardized to enable comparison between different laboratories with CHS, according to known reference values for each laboratory. All laboratories are operated by CHS and are under strict quality assurance. Blood lipid levels were the most recent available levels. All patients undergoing lipid levels analysis are routinely instructed to fast for 12 h before withdrawal of blood. We had no way of verifying that this practice was followed in a retrospective analysis of a computerized database. Indications for lipid level analysis were not available; however, the CHS participates in the National Program for Quality Indicators in Primary Care, supervised by the Ministry of Health. One of the indicators in this programme is testing of LDL-cholesterol every 5 years for enrollees over the age of 35 years. Currently, 86.2% of CHS enrollees over the age of 35 years have undergone LDL-cholesterol level analysis within the last 5 years (CHS, unpublished data). Because current lipid levels might reflect the effect of pharmacological or non-pharmacological therapy, a subset of patients without cardiovascular disease, hypertension or diabetes (the “low-risk subset”) was used for the comparison of lipid levels (Fig. 1).
Person-time was not available, as the date of diagnoses is not reliably registered in the database. Psoriasis patients and controls were selected randomly from all CHS practices, without matching of controls to patients regarding place of living or practices.
The proportions of patients with dyslipidaemia were compared between patients with and without psoriasis by univariate analyses, using χ2 tests to compare categorical parameters between the groups and t-tests for comparison of continuous variables. Logistic regression models were used to measure the association between psoriasis and dyslipidaemia in a multivariate analysis. For the “low-risk” subset, lipid levels were compared utilizing t-tests for univariate analysis and multiple linear regression models. Abnormal lipid levels were also analysed using dichotomous categories of abnormal total cholesterol (more than 200 mg/dl), LDL-cholesterol (over 130 mg/dl), triglyceride levels (over 200 mg/dl) and HDL-cholesterol (less than 40 mg/dl), based on the National Cholesterol Education Program Adult Treatment Plan III definitions (26). For this analysis, χ2 tests and logistic regression models were used for univariate and multivariate analyses, respectively. In all types of multivariate models, covariates were selected for multivariate analysis if the univariate p-value for the association between the potential confounder and dyslipidaemia was less than 0.1, and remained in the model if the multivariate p-value was less than 0.05. Statistical analysis was performed using SPSS software, version 13. The study was approved by the institutional review board of Soroka University Medical Center.
RESULTS
The study included 10,669 psoriasis patients and 22,996 controls with available lipid levels, and was over the age of 20 years. Psoriasis patients were older than controls (mean age: 57.8 vs. 54.8 years, p < 0.001), more likely to be male (49.3% vs. 41.1%, p < 0.001), and were more frequently diagnosed with other diseases associated with dyslipidaemia, such as smoking, diabetes, hypertension, obesity and hypothyroidism (Table I). Overall, dyslipidaemia was diagnosed among 57.1% of cases, compared with 47.4% of controls (p < 0.001; odds ratio (OR): 1.48, 95% confidence interval (CI): 1.40–1.55). Lipid levels among psoriasis patients and controls are listed in Table I.
Table I. Baseline characteristics of the study population (n = 33,665)
| Characteristic | Psoriasis patients (n = 10,669) | Controls (n = 22,996) | p-value |
| Age (years) mean ± SD Median (range) | 57.8 ± 15.6 58 (0–100) | 54.8 ± 17.9 55 (20–102) | < 0.001 |
| Female gender | 5,412 (50.7%) | 13,537 (58.9%) | < 0.001 |
| Current smoker | 2,897 (27.2%) | 4,415 (19.2%) | < 0.001 |
| Hypertension | 4,002 (37.5%) | 6,669 (29.0%) | < 0.001 |
| Diabetes | 2,112 (19.8%) | 3,492 (15.2%) | < 0.001 |
| Obesity | 2,560 (24.0%) | 4,109 (17.9%) | < 0.001 |
| Cardiovascular disease | 2,860 (26.8%) | 4,844 (21.1%) | < 0.001 |
| Hypothyroidism | 1,102 (10.3%) | 1,878 (8.2%) | < 0.001 |
| Psychiatric co-morbidity | 1,685 (15.8%) | 3,019 (13.1%) | < 0.001 |
| Residence in major citiesa | 4,158 (39.0%) | 8,794 (38.2%) | 0.199 |
| Residence in the peripheryb | 4,322 (40.5%) | 9,500 (41.3%) | 0.164 |
| Arab ethnicity | 847 (7.9%) | 3,435 (14.9%) | < 0.001 |
| Cholesterol, mean (mg/dl) | 195.5 ± 39.3 | 195.0 ± 40.0 | 0.273 |
| LDL-cholesterol, mean (mg/dl) | 117.2 ± 32.5 | 117.3 ± 32.8 | 0.867 |
| HDL-cholesterol, mean (mg/dl) | 48.3 ± 12.9 | 49.9 ± 13.4 | < 0.001 |
| Triglycerides, mean (mg/dl) | 148.8 ± 15.6 | 139.3 ± 86.1 | < 0.001 |
| Dyslipidaemia | 6,074 (56.9%) | 10,882 (47.3%) | < 0.001 |
aThree major cities in Israel (Tel Aviv, Jerusalem and Haifa).
bIn northern or southern Israel, compared with central Israel.
SD: standard deviation; LDL: low-density lipoproteins; HDL: high-density lipoproteins.
A multivariate logistic regression model demonstrated that psoriasis was associated with dyslipidaemia, even after controlling for confounders (Table II), though the strength of the association decreased (OR = 1.19, 95% CI: 1.12–1.26, p < 0.001, Table II).
It was suspected that lipid levels might reflect the effect of medical therapy, including lipid-lowering drugs. Indeed, when all subjects were included in the analysis, paradoxical negative associations between cardiovascular risk factors (diabetes, hypertension) or cardiovascular disease and lipid levels were found (data not shown). These associations probably reflect treatment with statins and fibrates. Therefore, analysis of lipid levels was restricted to a “low-risk” subset of patients without cardiovascular disease, diabetes and hypertension. This subset included younger patients (mean age, 49.5 ± 14.5 years among psoriasis patients and 46.3 ± 15.7 years among controls), who were more likely to be female (54% of psoriasis patients, 62% of controls), were less likely to smoke (25% and 17%, respectively), be obese (14% and 11%) and have hypothyroidism (8% and 6%) or psychiatric co-morbidity (11% and 9%) compared with the total study population (Table I). Significant differences in the age and gender distribution, as well as the prevalence of smoking, obesity, hypothyroidism and psychiatric illness were still noted in this subset of patients between psoriasis patients and controls.
Table II. Logistic regression for dyslipidaemia (n = 33,582)
| Variable | OR | 95% CI | p-value |
| Psoriasis | 1.19 | 1.12–1.26 | < 0.001 |
| Age (per year) | 1.04 | 1.03–1.05 | < 0.001 |
| Male gender | 1.10 | 1.04–1.17 | < 0.001 |
| Diabetes | 2.57 | 2.37–2.78 | < 0.001 |
| Hypertension | 1.50 | 1.40–1.60 | < 0.001 |
| Obesity | 1.53 | 1.43–1.64 | < 0.001 |
| Cardiovascular disease | 2.45 | 2.27–2.64 | < 0.001 |
| Current smoker | 1.56 | 1.47–1.66 | < 0.001 |
| Hypothyroidism | 1.47 | 1.34–1.61 | < 0.001 |
| Arab ethnicity | 0.74 | 0.68–0.80 | < 0.001 |
| Residence in major citiesa | 1.13 | 1.07–1.20 | < 0.001 |
| Residence in the peripheryb | 1.10 | 1.04–1.16 | < 0.001 |
aThree major cities in Israel (Tel Aviv, Jerusalem and Haifa).
bIn northern or southern Israel, compared with central Israel.
OR: odds ratio; CI: confidence interval. Place of residence and/or ethnicity were missing in 83 patients, hence the number of patients included in the model differs from that specified in Table I.
Lipid levels were analysed both as normal vs. abnormal (Table III), and as continuous variables (Table IV). While elevated LDL-cholesterol and triglycerides levels were associated with psoriasis in univariate analysis, these associations disappeared after controlling for confounders (Table III). Low HDL-cholesterol was associated with psoriasis even after controlling for covariates (Table III). Elevated total cholesterol was not associated with psoriasis either in univariate or multivariate analyses (Table III). When lipid levels were analysed as continuous variables, psoriasis was associated with higher total cholesterol, LDL-cholesterol and triglyceride levels and with lower HDL-cholesterol levels in univariate analysis (Table IV). After controlling for confounders, these associations retained statistically significant only for triglycerides and HDL-cholesterol (Table IV), although the differences were subtle.
Table III. Univariate and multivariate analysis for abnormal lipid levels (logistic regression models) (n = 18,860)
| Lipid level abnormality (mg/dl) | Psoriasis patients (n = 5266) n (%) | Controls (n = 13,594) n (%) | Univariate analysis | Multivariate analysis |
| OR (95% CI) | p-value | OR (95% CI) | p-value |
| Total cholesterol > 240 | 774 (14.7%) | 1,862 (13.7%) | 1.09 (0.99–1.19) | 0.075 | 1.01 (0.92–1.11)a | 0.838 |
| LDL > 130 | 1,831 (40.0%) | 4,292 (36.9%) | 1.15 (1.07–1.24) | < 0.001 | 1.05 (0.97–1.13)b | 0.214 |
| Triglycerides > 200 | 817 (15.9%) | 1,791 (13.5%) | 1.21 (1.10–1.33) | < 0.001 | 1.09 (0.99–1.20)c | 0.081 |
| HDL < 40 | 1,154 (24.9%) | 2,614 (21.9%) | 1.18 (1.08–1.28) | < 0.001 | 1.11 (1.02–1.21)c | 0.022 |
aControlled for age, gender, current smoking and residence in cities and in the periphery of Israel.
bControlled for age, gender, obesity, current smoking and residence in the periphery of Israel.
cControlled for age, gender, obesity, current smoking and Arab ethnicity.
LDL: low-density lipoproteins; HDL: high-density lipoproteins; OR: odds ratio; CI: confidence interval.
Table IV. Univariate and multivariate analysis for lipid levels (multiple linear regression models) (n = 18,860)
| Lipid category | Psoriasis patients (n = 5,266) (mg/dl) | Controls (n = 13,594) (mg/dl) | Univariate analysis p-value | Multivariate analysis |
| B for psoriasis | p-value |
| Total cholesterol | 200.3 ± 38.7 | 196.9 ± 40.1 | < 0.001 | +0.86a | 0.167 |
| LDL | 123.4 ± 32.0 | 120.6 ± 32.9 | < 0.001 | +0.78b | 0.158 |
| Triglycerides | 137.6 ± 77.0 | 130.2 ± 84.5 | < 0.001 | +2.69c | 0.045 |
| HDL | 49.8 ± 13.0 | 51.1 ± 13.6 | < 0.001 | –0.82d | < 0.001 |
aControlled for age, gender, obesity, current smoking, Arab ethnicity and residence in cities and in the periphery of Israel.
bControlled for age, gender, obesity, current smoking and residence in cities and in the periphery of Israel.
cControlled for age, gender, obesity, current smoking, Arab ethnicity and hypothyroidism.
dControlled for age, gender, obesity and Arab ethnicity.
LDL: low-density lipoproteins; HDL: high-density lipoproteins.
In a sensitivity analysis, we tested the hypothesis that excess dyslipidaemia prevalence in psoriasis patients was partly related to medication used to treat psoriasis. Acitretin and cyclosporine are used by 3.5% and 0.3% of psoriasis patients in CHS. We assumed all these patients were included in the group with dyslipidaemia. Therefore, we subtracted 405 patients (3.8%) from the group with dyslipidaemia. As a result, the prevalence of dyslipidaemia in psoriasis patients decreased slightly (55.2% vs. 47.4% of controls, p < 0.001) and the crude OR somewhat decreased (1.37, 95% CI 1.31–1.44).
DISCUSSION
The present study is a population-based cross-sectional study, based on a large sample of patients with psoriasis and controls from the CHS database. Psoriasis was found to be associated with a higher prevalence of dyslipidaemia. After controlling for confounders, psoriasis patients had a higher prevalence of dyslipidaemia, higher triglycerides levels and lower HDL levels. However, associations with total cholesterol and LDL were not statistically significant in the multivariate analysis.
In the present study psoriasis was associated with dyslipidaemia. The association between psoriasis and dyslipidaemia is somewhat controversial, with inconsistent findings. Most studies (3, 6, 17–20, 26) included very small sample sizes, and few (5, 13) were based on large population-based registries. OR for dyslipidaemia were reported to range from 1.04 (13) to 3.76 (16). The association with dyslipidaemia seems to be stronger in patients with psoriatic arthritis and more severe disease (6, 16). In other studies, cholesterol levels in psoriasis patients were found to be either higher (6, 18, 19), similar (11, 17, 20, 21) or even lower (3). LDL levels are reported to be higher (6, 18, 19), or similar (3, 11, 17, 20, 21) to controls. Triglyceride levels were previously reported to be higher in psoriasis patients in some studies (3, 6, 18, 20), but not in other studies (11, 17, 19, 21). HDL levels were previously reported to be either lower (6, 17, 18, 20), similar (19, 21) or higher (3, 11) among psoriasis patients.
Several mechanisms for the increased lipid levels in psoriasis have been suggested. Psoriasis is a chronic inflammatory state (1), and chronic inflammation has been suggested as part of the metabolic syndrome. Both psoriasis and the metabolic syndrome are characterized by increases in the immunological activity of type 1 helper T cells. Cytokines such as TNF-α and interleukin-6 seem to play a central role. TNF may lead to insulin resistance by inhibiting insulin-mediated tyrosine phosphorylation of the insulin receptor, as well as insulin receptor substrate-1. TNF-α has also been shown to be a potent activator of c-Jun amino-terminal kinase, which stimulates activator protein-1, a major regulator of pro-inflammatory activity (13, 16, 21). Mouse models show that c-Jun amino-terminal kinase activity is abnormally elevated in obesity, while its absence is associated with decreased adiposity, improved insulin sensitivity and enhanced insulin receptor signalling (13). A potential beneficial increase of HDL occurs when using TNF-α inhibitors (4).
Another explanation for the tendency of psoriasis patients to develop metabolic syndrome might be related to an unhealthy lifestyle, including poor eating habits, alcohol consumption, stress, and decreased exercise, which may lead to development of increased body weight and the metabolic syndrome (13).
In addition, the metabolic syndrome itself could predispose an individual to developing psoriasis, as observed in a case-control study in which obesity was reported to be a risk factor for psoriasis (12, 13). Auto-antibodies recognizing oxidized LDL have been found in psoriasis. The lipid abnormalities seen in psoriasis might facilitate and maintain the inflammatory reaction in the skin. The level of antibodies against oxidized LDL is reported to correlate with disease severity (11, 27). Therapy with statins may be beneficial to patients with psoriasis, as these reduce LDL oxidation and may even have immunomodulatory activities that may improve the psoriasis skin and cause a shift from pro-inflammatory to anti-inflammatory conditions in psoriasis (4).
Finally, some medications used to treat psoriasis, such as oral retinoids and cyclosporine, may induce dyslipidaemia in some patients (13, 21), including hypercholesterolemia, hypertriglyceridaemia and low HDL-cholesterol (4). While no data on medical therapy for psoriasis was available in the current study, patients treated with oral retinoids and cyclosporine are a small minority of CHS enrollees. In a sensitivity analysis, the association between psoriasis and dyslipidaemia persisted even after eliminating these patients.
The present study has some potential limitations. Directionality of the association cannot be established by the study design. No information on lipid-lowering drugs or systemic medication for psoriasis was available. We also had no information regarding lipid levels at the time of diagnosis. Analysis of lipid levels was limited to patients without hypertension and diabetes mellitus; therefore, differences between psoriasis and controls might be underestimated. Lipid levels were more likely to be available for psoriasis patients than for controls. Indications for lipid levels analysis were not available. While most of the patients (including controls) were probably monitored for lipid levels as part of the National Program for Quality Indicators in Primary Care, a selection bias cannot be completely excluded. While no matching for the year of measurement was performed, there is no reason to believe a difference in timing of blood tests between psoriasis and controls was responsible for the difference detected, although this possibility cannot be ruled out.
To conclude, an association between psoriasis and dyslipidaemia was noted. Further prospective studies are needed to establish our observation. Nevertheless, we suggest that psoriasis has a role as a new risk factor for dyslipidaemia. This study supported the claim that psoriasis might be associated with dyslipidaemia, and it is therefore prudent to follow-up psoriasis patients for the development of cardiovascular risk factors (7).
REFERENCES
1. Langley RG, Krueger GG, Griffiths CE. Psoriasis: epidemiology, clinical features, and quality of life. Ann Rheum Dis 2005; 64 Suppl 2: ii18–ii23.
2. Schon M, Henning-Boehricke W. Psoriasis. N Engl J Med 2005; 352: 1899–1912.
3. Pietrzak A, Lecewicz-Torun B. Activity of serum lipase (EC 3.1.1.3) and the diversity of serum lipid profile in psoriasis. Med Sci Monit 2002; 8: CR9–CR13.
4. Wakkee M, Thio HB, Prens EP, Sijbrands EJ, Neumann HA. Unfavorable cardiovascular risk profiles in untreated and treated psoriasis patients. Atherosclerosis 2007; 190: 1–9.
5. Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA 2006; 296: 1735–1741.
6. Rocha-Pereira P, Santos-Silva S, Rebelo I, Figueredo A, Quintanilha A, Teixeira F. Dislipidemia and oxidative stress in mild and in severe psoriasis as a risk for cardiovascular disease. Clin Chim Acta 2001; 303: 33–39.
7. Christophers E. Comorbidities in psoriasis. J Eur Acad Dermatol Venereol 2006; 20: 52–55.
8. Henseler T, Christophers E. Disease concomitance in psoriasis. J Am Acad Dermatol 1995; 32: 982–986.
9. Mallbris L, Akre O, Granath F, Yin L, Lindelöf B, Ekbom A, et al. Increased risk for cardiovascular mortality in psoriasis inpatients but not in outpatients. Eur J Epidemiol 2004; 19: 225–230.
10. Mallbris L, Ritchlin CT, Ståhle M. Metabolic disorders in patients with psoriasis and psoriatic arthritis. Curr Rheumatol Rep 2006; 8: 355–363.
11. Mallbris L, Granath F, Hamsten A, Ståhle M. Psoriasis is associated with lipid abnormalities at the onset of skin disease. J Am Acad Dermatol 2006; 54: 614–621.
12. Naldi L, Chatenoud L, Linder D, Belloni Fortina A, Peserico A, Virgilli AR, et al. Cigarette smoking, body mass index, and stressful life events as risk factors for psoriasis: results from an Italian case-control study. J Invest Dermatol 2005; 125: 61–67.
13. Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB, Gelfand JM. Prevalence of cardiovascular risk factors in patients with psoriasis. J Am Acad Dermatol 2006; 55: 829–835.
14. Pearce DJ, Morrison AE, Higgins KB, Crane MM, Balkrishnan R, Fleischer AB Jr, et al. The comorbid state of psoriasis patients in a university dermatology practice. J Dermatolog Treat 2005; 16: 319–323.
15. Shapiro J, Cohen AD, David M, Hodak E, Chodik G, Viner A, et al. The association between psoriasis, diabetes mellitus, and atherosclerosis in Israel: a case-control study. J Am Acad Dermatol 2007; 56: 629–634.
16. Sommer DM, Jenisch S, Suchan M, Christophers E, Weichental M. Increased prevalence of the metabolic syndrome in patients with moderate to severe psoriasis. Arch Dermatol Res 2006; 298: 321–328.
17. Reynoso-von Drateln C, Martinez-Abundis E, Balcazar-Munoz RB, Bustos-Saldana R, Gonzalez-Ortiz M. Lipid profile, insulin secretion, and insulin sensitivity in psoriasis. J Am Acad Dermatol 2003; 48: 882–885.
18. Tekin NS, Tekin IO, Barut F, Sipahi EY. Accumulation of oxidized low-density lipoprotein in psoriatic skin and changes of plasma lipid levels in psoriatic patients. Mediators Inflamm 2007; 2007: 78454.
19. Piskin S, Gurkok F, Ekuklu G, Senol M. Serum lipid levels in psoriasis. Yonsei Med J 2003; 44: 24–26.
20. Vahlquist C, Michaëlsson G, Vessby B. Serum lipoprotein in middle-aged men with psoriasis. Acta Derm Venereol 1987; 67: 12–15.
21. Farshichian M, Zamanian A, Farshichian M, Monsef AR, Mahjub A. Serum lipid levels in Iranian patients with psoriasis. J Eur Assoc Deramatol Venereol 2007; 21: 802–805.
22. Cohen AD, Shapiro Y, Davidovici B, Meyerovitch J, Vidavsky L, Vardy DA, et al. Psoriasis and ischemic heart disease: a case-control study. Giornale Iraliano di Dermatolgia e Venereologia 2007; 142: 299–302.
23. Cohen AD, Dreiher J, Shapiro Y, Vidavsky L, Vardy DA, Davidovici B, et al. Psoriasis and diabetes. A population-based cross-sectional study. J Eur Acad Dermatol Venereol 2008; 22: 585–589.
24. Rennert G, Peterburg Y. Prevalence of selected chronic diseases in Israel. Isr Med Assoc J 2001; 3: 404–408.
25. Vinker S, Fogelman Y, Elhayany A, Nakar S, Hahan E. Usefulness of electronic databases for the detection of unrecognized diabetes patients. Cardiovasc Diabetol 2003; 2: 13.
26. NCEP. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) – final report. NIH publication No. 02-5215, USA 2002.
27. Vanizor Kural B, Orem A, Cimsit G, Yandi YE, Calapoglu M. Evaluation of the atherogenic tendency of lipids and lipoprotein content and their relationship with oxidant-antioxidant system in patients with psoriasis. Clin Chim Acta 2003; 328: 71–82.