We describe here a 50-year-old Japanese man with nephrogenic systemic fibrosis. He had been suffering from chronic renal insufficiency and had been treated with haemodialysis. He had undergone magnetic resonance angiography using gadodiamide 7 years previously. One month after magnetic resonance angiography, he noted swelling, hotness, induration and pain in his left arm. The same symptoms gradually spread over his lower extremities, resulting in flexion contractures with limited range of motion. Physical examination revealed skin sclerosis on his extremities with a glossy brownish skin surface. Histologically, increased collagen fibres with high cellularity were seen in the dermis and subcutaneous septa. Thickened fascia was also noted, as well as osseous metaplasia under the fascia. Computed tomography of the whole body revealed multiple calcification of the fascia in many muscles. Treatment with intravenous sodium thiosulphate did not result in any clinical improvement. Key words: nephrogenic systemic fibrosis; gadolinium; calcification; osseous metaplasia; sodium thiosulphate.
(Accepted May 9, 2008.)
Acta Derm Venereol 2008; 88: 597–600.
Yayoi Nagai, Department of Dermatology, Gunma University Graduate School of Medicine, 3-39-22, Showamachi, Maebashishi, Gunma 371-8511, Japan. E-mail yanagai@showa.gunma-u.ac.jp
Nephrogenic systemic fibrosis (NSF) is a rare disease that has been described with increasing frequency in the medical literature. This entity was recognized in several patients in 1997, and first reported in the literature in 2000 (1). NSF is characterized by skin indurations that affect the extremities in patients with renal failure. It was originally termed nephrogenic fibrosing dermopathy (NFD) because this fibrosing skin condition occurred exclusively in patients with renal failure and the symptoms were thought to be limited to the skin. Subsequently, autopsies of patients with the disease revealed systemic involvement including fibrosis of the lungs, pleura, pericardium, myocardium, kidney, muscle, bone, testis and dura (2, 3). Therefore, “nephrogenic systemic fibrosis” is now the preferred terminology. Recently, several studies support the theory that gadolinium-based contrast agents play a causative role in the development of NSF (4–12). We report here a patient with NSF showing multiple calcifications and osseous metaplasia.
Case report
A 44-year-old man with an 8-year history of end-stage renal disease due to glomerulonephritis underwent renal transplantation in 2000. However, 4 days later, urgent haemodialysis was restarted due to anuria. Magnetic resonance angiography (MRA) using intravenous administration of gadodiamide (15 ml) demonstrated arterial anastomotic stenosis. Approximately one month after the MRA was performed, the patient noted swelling, hotness, indurations and pain in his left arm, resulting in flexion contractures with limited range of motion. These symptoms gradually spread over the lower extremities, followed by multiple joint contractures including the shoulders, wrists, knees and ankles. At that time, no calcification was noted in the X-rays of the extremities. His symptoms, including skin sclerosis and flexion contractures, had gradually worsened.
At the age of 50 years in 2006, while he was hospitalized in a general hospital because of a fracture of the humerus, the diagnosis of NSF was established by one of the authors (Tsushima) based on the clinical and histological findings and the history of having had MRA using gadodiamide. At that time, 7 years had passed since the onset of NSF.
He was hospitalized in our department for treatment on 27 June 2007. The laboratory findings, haematology, C-reactive protein (CRP), erythrocyte sedimentation rate, transaminase and creatine kinase levels were within normal limits. Increased eosinophils were not detected. Serum calcium and phosphate levels were normal. Anti-nuclear antibodies as well as antibodies to Scl-70, centromere, U1-RNP and SS-A/B antibodies were all negative. Physical examination revealed skin swelling and sclerosis of the arms, especially in the left forearm, where an arteriovenous fistula was made for haemodialysis (Fig. 1a). His legs showed a glossy, smooth surface with brownish colour changes (Fig. 1b). Sclerotic induration was palpated in the deep part of the skin, and pinching of the superficial skin was possible. The patient was disabled, mainly as a result of severe flexion joint contractures in the left wrist, both knees and ankles and he could hardly walk by himself. There was no skin sclerosis in his face, neck and trunk. Since bony masses were palpated in the deep part of his sural lesions, we performed a biopsy from that lesion.
Fig. 1. (a) Physical examination revealed swelling and skin sclerosis of the arms, especially in left forearm where arteriovenous fistula was made. (b) Both legs showed a glossy, smooth surface with brownish changes in colour. Skin sclerosis was palpated in the deep part of the skin.
Histological findings revealed increased collagen fibres throughout the dermis, with cellular infiltration consisting mainly of plump spindle cells (Fig. 2 a, b). Immunohistochemically, CD34-positive spindle-shaped cells were prominent. Such findings were almost the same as those of his left forearm. The fascia was also fibrotic and widened. Furthermore, the notable change was osseous metaplasia under the fascia with mineralized and unmineralized woven bone. Degenerated muscle fibres were seen adjacent to the ossificated area (Fig. 2c).
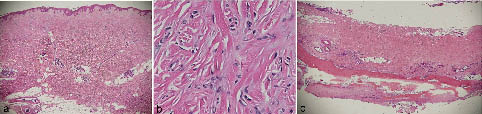
Fig. 2. (a) Biopsy of the skin and muscles from a hard massive nodule in the patient’s right lower extremity. Widened and increased collagen fibres were seen in the dermis. (b) High magnification shows cellular infiltration consisting especially of plump spindle cells with CD34 positivity. (c) The fascia was also fibrotic and widened. Notable changes included osseous metaplasia under the fascia. Degenerated muscle fibres were also noted adjacent to the bone tissue.
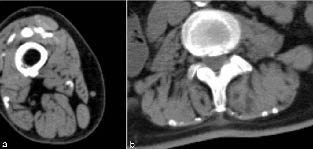
Computed tomography of the whole body demonstrated high attenuation of the fascia and muscles representing calcinosis, which was widely distributed in the muscles in his trunk and extremities, such as the erector muscles of the spine, the muscles gluteus medius, sartorius quadriceps, gastrocnemius and biceps femoralis muscles (Fig. 3).
Fig. 3. Computed tomography findings of (a) the quadriceps muscles and (b) elector muscles of the spine. High attenuation of the fascia and muscles are noted, representing calcinosis.
Since psoralen plus ultraviolet A (PUVA) therapy was not effective, intravenous infusion of sodium thiosulphate (STS) was administered based on a recent report (12). Treatment was started at a dose of 2 g/day every other day after the dialysis. However, when the dose of STS was increased to 10 g/day, the treatment was discontinued due to decreased levels of platelets. We restarted the treatment at STS 8 g/day after a 3-week interval, at which time platelet counts returned to normal. Although the patient could be treated with STS for 3 months without further adverse effects, he did not obtain any successful result.
Discussion
NSF is characterized clinically by acute onset of hardening and thickening of the skin on the extremities and trunk, often resulting in flexion contractures. It develops only in patients with renal insufficiency. Histologically, an increase in spindle-shaped cells, collagen fibres, and sometimes mucin deposition in the dermis, have been demonstrated (1, 13). The clinical features of established cutaneous lesions resemble those of both systemic sclerosis (SSc) and diffuse fasciitis. However, Raynaud’s phenomenon and sclerodactyly, common symptoms in patients with SSc, are absent in NSF. Histological features of thickened homogenous collagen fibres and sparse cellular infiltration in the dermis of patients with SSc distinguish it from NSF. In addition, antinuclear antibodies are positive in most of the SSc patients. Patients with eosinophilic fasciitis can show swelling and induration of the extremities; however, histological findings reveal deep fascial inflammation and eosinophilic infiltration, which are distinguishable from those of NSF.
Muscle involvement has been reported in severely affected patients (3, 14–17). Mendoza et al. (3) reported that some patients showed severe woody indurations in the muscles of the legs, thighs and forearms; however, true muscle weakness was not present. Muscle involvement in patients with NSF has been detected by abnormal scintigraphy, showing increased uptake of Tc-hydroxymethylene diphosphonate in the skeletal muscle underlying the involved skin. This finding supports that the abnormal process may extend deeper than the dermis (17). Histologically, affected muscles revealed mild to severe fibrosis, degenerated fibres and inflammatory cells.
One of the typical findings in our case was ossification adjacent to the fascia and muscles in both lower legs. Patients with NSF have frequently been reported to show a spectrum of abnormal calcification in the dermis and subcutis (18–20), ranging from the expected dystrophic calcinosis cutis, benign nodular calcifications, and metastatic calcinosis cutis that occur in patients with renal disease, to a very unusual case of osseous metaplasia in NSF lesions (21). Some authors have proposed that calcification may be a part of the disease spectrum (19, 21). In an autopsy case, extensive calcification and fibrosis of the diaphragm and psoas muscles were described (14). Ruiz-Genao et al. (21) reported a very extensive osseous metaplasia in the superficial dermis with formation of islands and spicules of mineralized and unmineralized woven bone surrounded by osteoblasts and scattered osteoclasts. Hershko et al. (22) suggested that the coexistence of osteoclast-like giant cells and increased fibrosis may be attributed to the elevated TGF-beta levels in patients with NSF. In our patient, multiple calcifications in the fascia and muscles were noted along with osseous metaplasia. Metaplastic ossification can be regarded as a peculiar histological feature of a subset of NSF patients, especially in the late stages of the disease.
In 2006, Grobner (4) first pointed out the relationship between gadolinium-based contrast agents and NSF. Since then, subsequent reports have supported his suggestion (4–12). Even though some associated factors, such as altered kidney function and inflammatory burden, may be involved, there is no doubt that gadodiamide was used in the majority of patients with NSF reported in the literature. Recently, two groups documented the deposition of gadolinium in biopsy specimens using electron-dispersion spectroscopy (5, 6). In vivo, the gadolinium ion is bound to a particular chelate. All clinically available gadolinium-based contrast agents have been shown to be extremely stable in vitro. The stability of the gadolinium-based agents depends on multiple factors including the thermodynamic stability constant, solubility constant, selectivity constant. Marckmann et al. (7) have postulated that NSF may result from a toxic reaction from free gadolinium (Gd3+), liberated from the chelate, which is not adequately excreted due to impaired renal function. Furthermore, it is speculated that the gadolinium retained in the tissues is phagocytosed by macrophages, as all the gadolinium identified in the tissue samples is associated with cell bodies. This phagocytosed gadolinium may generate profibrotic cytokines and/or growth factors that ultimately result in dermal or systemic fibrosis (6).
The treatment modalities attempted so far include plasmapheresis, extracorporeal photopheresis, cyclosporin, tacrolimus, intralesional triamcinolone, intralesional methotrexate, interferon-alpha and local PUVA therapy (14). Several reported cases showed improvement with one of these treatments; however, most of these treatments did not result in much improvement. In 2007, Yerram et al. (12) reported a patient with 2 years’ disease history who demonstrated marked improvement in pain and skin changes after treatment with intravenous STS. It is possible that STS may chelate Gd3+ and enhance its solubility and stability in serum, thereby facilitating its excretion during dialysis. If the Gd3+ precipitated in the tissue could trigger fibrosis in NSF, its removal would improve our patient’s condition. Therefore, we introduced STS as part of our patient’s treatment regimen. However, this did not result in any significant changes, although the scheduled dosage (25 g/day) was never reached due to a decrease in platelet count. In addition, Yerram’s case with remarkable improvement had suffered from NSF for only 2 years (12). The difference in STS dose and disease duration may account for the poor clinical outcome in our patient.
NSF is a new disease entity and has become well recognized. Although many cases have been reported in Europe and the USA, only eight cases including our patient have been reported in Japan. It is not known whether there is a racial difference or whether this is due to the lack of recognition of this disease in Japan. Dermatologists should be aware of this unique disease. Correct and expedient diagnosis of NSF may be critical to obtain a better outcome by treating patients in the early stages of the disease.
References
1. Cowper SE, Robin HS, Steinberg SM, Su LD, Gupta S, Leboit PE. Scleromyxoedema-like cutaneous diseases in renal-dialysis patients. Lancet 2000; 356: 1000–1001.
2. Ting WW, Stone MS, Madison KC, Kurtz K. Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol 2003; 139: 903–939.
3. Mendoza F, Arflett CM, Sandorfi N, Latinis K, Piera-Velazquez S, Jimenez SA. Description of twelve cases of nephrogenic fibrosing dermopathy and review of the literature. Semin Arteritis Rheum 2006; 35: 238–249.
4. Grobner T. Gadolinium – a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant 2006; 21: 1104–1108.
5. Boyd AS, Zic JA, Abraham JL. Gadolinium deposition in nephrogenic fibrosing dermopathy. J Am Acad Dermatol 2007; 56: 27–30.
6. High WA, Ayers RA, Chandler J, Zito G, Cowper SE. Gadolinium is detectable within the tissue of patients with nephrogenic systemic fibrosis. J Am Acad Dermatol 2007; 56: 21–26.
7. Marckmann P, Skov L, Rossen K, Dupont A, Damholt MB, Heaf JG, Thomsen HS. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast enhanced magnetic resonance imaging. J Am Soc Nephrol 2006; 17: 2359–2362.
8. Thomsen HS, Morcos SK, Dawson P. Is there a causal relation between the administration of gadolinium based contrast media and the development of nephrogenic systemic fibrosis (NSF)? Clin Radiol 2006; 61: 905–906.
9. Kuo PH, Kanai E, Abu-Alfa AK, Cowper SE. Gadolinium-based MR contrast agents and nephrogenic systemic fibrosis. Radiology 2007; 242: 647–649.
10. Richmond H, Zwerner J, Kim Y, Fiorentino D. Nephrogenic systemic fibrosis. Arch Dermataol 2007; 143: 1025–1030.
11. Pryor JG, Poggioli G, Galatia N, Gust A, Robison J, Samic F, et al. Nephrogenic systemic fibrosis: a clinicopathologic study of six cases. J Am Acad Dermatol 2007; 57: 105–111.
12. Yerram P, Saab G, Karuparthi PR, Hayden MR, Khanna R. Nephrogenic systemic fibrosis: a mysterious disease in patients with renal failure – role of Gadolinium-based contrast media in causation and the beneficial effect of intravenous sodium thiosulfate. Clin J Am Soc Nephrol 2007; 2: 258–263.
13. Cowper SE, Su L, Robin H, Bhawan J, Leboit PE. Nephrogenic fibrosing dermopathy. Am J Dermatopathol 2001; 23: 383–393.
14. Introcaso CE, Hivnor C, Cowper S, Werth VP. Nephrogenic fibrosing dermopathy/nephrogenic systemic fibrosis: a case series of nine patients and review of the literature. Int J Dermatol 2007; 46: 447–452.
15. Levine JM, Taylor RA, Elman LB, Bird SJ, Lavi E, Stolzenberg ED, et al. Involvement of skeletal muscle involvement in dialysis-associated systemic fibrosis (nephrogenic fibrosing dermopathy) Muscle Nerve 2004; 30: 569–577.
16. Evenepoel P, Zeegers M, Segaert S, Claes K, Kuypers D, Maes B, et al. Nephrogenic fibrosing dermopathy: a novel, disabling disorder in patients with renal failure. Nephrol Dial Transplat 2004; 19: 469–473.
17. Gremmels J, Kirk G. Two patients with abnormal skeletal muscle uptake of Tc-99m hydroxymethylene diphosphonate following liver transplant; nephrogenic fibrosing dermopathy and graft vs host disease. Clin Nucl Med 2004; 29: 694–697.
18. Taylor E, Henderson J, Rennke H, Magee CC. Traumatic calsinosis cutis in a dialysis patient. Am J Kidney 2004; 44: 18–21.
19. Edsall L, English J, Teague M, Patterson JW. Calciphylaxis and metastatic calcification associated with nephrogenic fibrosing dermopathy. J Cutan Pathol 2004; 31: 247–253.
20. Lewis KG, Lester BW, Pan TD, Robinson-Bostom L. Nephrogenic fibrosing dermopathy and calciphylaxis with pseudoxanthoma elasticum-like changes. J Cutan Pathol 2006; 33: 695–700.
21. Ruiz-Genao D, Pascual-Lopez M, Fraga S, Aragues M, Garcia-Diez A. Osseous metaplasia in the setting of nephrogenic fibrosing dermopathy. J Cutan Pathol 2005; 32: 172–175.
22. Hershko K, Hull C, Ettefagh L, Nedorost S, Dyson S, Horn T, Gilliam AC. A variant of nephrogenic fibrosing dermopathy with osteoclast-like giant cells: a syndrome of dysregulated matrix remodelling? J Cutan Pathol 2004; 31: 262–265.