Satoshi Nakagawa1, Hachiro Tagami2, Ryo Ichinohasama3 and Setsuya Aiba2
1Department of Dermatology, Public Soma General Hospital, Tsubogasaku 142, Niinuma, Soma 976-8686, Departments of 2Dermatology and 3Hematopathology, Tohoku University Graduate School of Medicine, Sendai, Japan. E-mail: n-derma@bb.soma.or.jp
Accepted May 2, 2008.
Sir,
Myeloid sarcoma, or granulocytic sarcoma, is a lesion characterized by the presence of one or more tumour masses, consisting of myeloblasts or immature myeloid cells, in sites other than the bone marrow. The sites for predilection are the skin, lymphoid tissue (lymph node, tonsil), subperiostal bone (skull, orbit, ribs), reproductive organs (testis ovary), gastrointestinal tract (intestine), central nervous system, etc. The skin lesion is known under the name of leukemia cutis. It sometimes is associated with myeloproliferative disorders, such as myelofibrosis. We present here a case of myeloid sarcoma with unusual skin manifestation.
CASE REPORT
An 85-year-old man presented with a 3-week history of rapidly-evolving multiple nodules on the trunk and limbs. He had been on medication for angina pectoris and nephrotic syndrome, and had been diagnosed as having myelofibrosis one year previously. On examination, there were numerous, soft, non-tender, pinkish, elevated nodules, 5–20 mm in diameter, on the trunk and extremities (Fig. 1). In addition, there was one 40 mm dome-shaped violaceous tumour on his right forearm. Laboratory studies revealed anaemia (haemoglobin; Hb 7.4 g/dl, normal ranges 12.0–16.0), leukopaenia (white blood cell count; 1700/μl, normal ranges 4000–8000), and renal dysfunction (blood area nitrogen 36.9 mg/dl, normal ranges 8–22 and creatinine 1.85 mg/dl, normal ranges 0.4–1.1). Analysis by computed tomography (CT) scanning revealed no specific changes, and bone-marrow biopsy showed only the features of myelofibrosis. Skin biopsy showed a dense, diffuse infiltrate of monomorphous medium-sized atypical monocytoid cells in the upper to mid dermis (Fig. 2). No epidermotropism was observed. Immunohistochemical studies revealed the presence of cells positive for CD4, CD45, CD56, CD68 (both KP1 and PGM1 antibodies), CD99 antigens and myeloperoxidase (in some tumour cells), but negative for CD2, CD3, CD5, CD7, CD10, CD20, CD30, CD34, CD57, CD79a, CD117, anaplastic lymphoma kinase, epithelial membrane antigen, granzyme B, and neutrophil elastase. The Ki-67 score was approximately 70%. Southern blot analysis of the DNA showed germ-line configuration for both T-cell receptor beta-chain and the immunoglobulin heavy chain. The patient was diagnosed with Myeloid sarcoma and hospitalized due to general fatigue and recurrent fever. Because the bone-marrow aspiration, performed one month after the skin biopsy, revealed the blastic cell infiltration of acute myeloid lymphoma (AML), we started chemotherapy with cytarabine ocfosfate. However, the patient died suddenly of a heart attack one week later, at which time the skin lesions had neither progressed nor regressed.
Fig. 1. Numerous flesh-coloured nodules on the trunk and the arm.
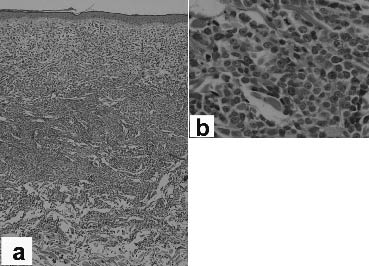
Fig. 2. Histopathological findings of the nodular lesion. (a) Dense, diffuse dermal infiltration of atypical cells. Tumour cells were medium-sized with high nuclear/cytoplasmic ratio and prominent nucleoli. (b) Some mitotic figures were present. (Haematoxylin and eosin, (a) ×40 and (b) ×400).
DISCUSSION
Myeloid sarcoma is usually presented as a single mass, although myeloid sarcoma with multiple skin lesions have been reported (1–3). The present case is unique because so many cobblestone-like skin lesions rapidly developed in such a short period of time over the trunk and limbs. Among the reviewed 92 cases of myeloid sarcoma (4), 25% of the patients developed de novo disease, and other cases had AML, myeloproliferative disorder, or myelodysplastic syndrome simultaneously (32%), or previously (35%). Because immunohistochemically myeloid sarcoma cells express various differentiation markers such as CD68/KP1, myeloperoxidase, CD117, CD99, CD68/PG-M1, CD34, terminal-deoxy-nucleotidyl-transferase and CD56, they are subdivided into seven categories: undifferentiated, blastic, differentiated, trilinear, with megakaryocytic differentiation, monoblastic, and myelomonocytic (4). Accordingly we diagnosed this case as myeloid sarcoma of monoblastic variant (CD68+, myeloperoxidase–, CD34–) in majority, with blastic variant (CD68+/–, myeloperoxidase+, CD34+/–) in minor population. More than 50% of the monoblastic myeloid sarcoma is reported to have skin manifestation, as in our case (2, 4). To start prompt treatment for myeloid sarcoma, it is mandatory to conduct immunophenotyping in order to make a precise diagnosis and to exclude the possibility of other lymphoproliferative disorders, such as acute lymphoblastic lymphoma, diffuse large B-cell lymphoma, or blastic natural killer (NK) cell lymphoma (plasmacytoid dendritic cell precursor tumour) (5). Among them, it is sometimes difficult to discriminate myeloid sarcoma from blastic NK cell lymphoma, because both may express common antigens (CD4, CD43, CD45, CD56, CD68) and because a myelomonocytic precursor cell might be an origin for blastic NK cell lymphoma (6). In our case, the finding that myeloperoxidase was positively-stained in a small population of the tumour cells, in addition to the patient’s medical history of myelofibrosis existing one year before the onset of the skin lesions, was helpful in making the diagnosis.
references
1. Long JC, Mihm MC. Multiple granulocytic tumors of the skin: report of six cases of myelogenous leukemia with initial manifestations in the skin. Cancer 1977; 39: 2004–2016.
2. Ohno S, Yokoo T, Ohta M, Yamamoto M, Danno K, Hamato N, et al. Aleukemic leukemia cutis. J Am Acad Dermatol 1990; 22: 374–377.
3. Fridus SR, Rodman OG, Cyran SJ 3rd, Cardelli MB. Multiple papules and plaques in a patient with ovarian carcinoma: granulocytic sarcoma (GS) of the skin. Arch Dermatol 1993; 129: 775, 778.
4. Pileri SA, Ascani S, Cox MC, Campidelli C, Bacci F, Piccioli M, et al. Myeloid sarcoma: clinico-pathologic, phenotypic and cytogenetic analysis of 92 adult patients. Leukemia 2007; 21: 340–350.
5. Petrella T, Bagot M, Willemze R, Beylot-Barry M, Vergier B, Delaunay M, et al. Blastic NK-cell lymphomas (agranular CD4+CD56+ hematodermic neoplasms). Am J Clin Pathol 2005; 123: 662–675.
6. Vermi W, Facchetti F, Rosati S, Vergoni F, Rossi E, Festa S, et al. Nodal and extranodal tumor-forming accumulation of plasmacytoid monocytes/interferon-producing cells associated with myeloid disorders. Am J Surg Pathol 2004; 28: 585–595.