Woon-Kyong Chung1, Heungsup Sung2, Mi-Na Kim2, Mi-Woo Lee1*, Jong-Hee Shin3, Jee-Ho Choi1, Kee-Chan Moon1 and Jai-Kyoung Koh1
Departments of 1Dermatology and 2Laboratory Medicine, University of Ulsan College of Medicine, Asan Medical Center, 388-1 Pungnapdong, Songpagu, Seoul, 138-736 and 3Department of Laboratory Medicine, Chonnam National University Medical School, Gwangju, Korea. *E-mail: 1052_hihi@hanmail.net
Accepted June 2, 2009.
Sir,
Scopulariopsis, which is a genus of non-dermatophytic filamentous fungi, contains a number of common saprophytic fungi found in soil, vegetables, air, and organic waste. To date, eight species of Scopulariopsis have been reported to cause human infections. Of these, S. brevicaulis is the most common; although is not generally considered to be a skin pathogen, the organism is isolated relatively frequently from onychomycosis patients (1). However, deeper cutaneous infection caused by S. brevicaulis is extremely rare. We describe here a woman with treatment-resistant S. brevicaulis facial infection after a filler injection performed by an unlicensed practitioner.
CASE REPORT
A 42-year-old woman presented in June 2008 with an ulcer covered by a black crust and surrounding palpable tender nodules on the right temple (Fig. 1). In September 2006, she had received collagen injections into both temples, administered by an unlicensed practitioner. About 6 months later, she detected palpable nodules on both temples. She visited the unlicensed practitioner again, and received intralesional injections of an unknown material (described as a neutralizing agent) into both temples. Thereafter, her face became gradually more swollen, and an ulcer developed on her right temple. The patient was otherwise healthy, and routine laboratory tests, including blood tests and a chest roentgenogram, yielded data within normal limits.
Fig. 1. A black-crusted ulcer with surrounding palpable tender nodules on the right temple.
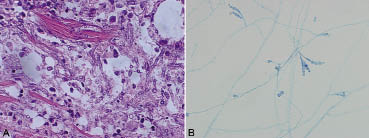
A skin biopsy was performed of a palpable nodule beside the crusted ulcer. Histology disclosed numerous branching septated hyphae and conidia in the deep dermis and subcutaneous fat (Fig. 2a). Fungal culture revealed entire-edged flat colonies with powdery, buff-to-brown, rugose surfaces. The reverse of the specimen culture was more waxy and yellow-white in colour. Lactophenol cotton blue mounts revealed numerous branching and septated hyphae with conidiophores and conidia in basipetal chains (Fig. 2b). As a Scopulariopsis infection was suspected, internal transcribed spacer (ITS) sequencing was performed to identify the isolate. An ABI PRISM 3130xl genetic analyser (Applied Biosystems, Foster City, CA, USA) and a Big-Dye Terminator Cycle Sequencing kit (Applied Biosystems) were employed. We found 100% homology with S. brevicaulis IFM 54315 (GenBank accession no. AB363754) and 99.5% (593 bp/596 bp) homology with S. brevicaulis CTSP F6 (GenBank accession no. EU862178) (2). Because the species showing the next-best homology (98.7%) was S. flava (GenBank accession no. AY494711), we identified the isolate as S. brevicaulis (Fig. 3S, http://adv.medicaljournals.se/article/abstract/ 10.2340/00015555-0713/fig3) (2).
Fig. 2. (a) Numerous branching septated hyphae and conidia in the deep dermis and subcutaneous fat (haematoxylin and eosin (H&E) stain, original magnification ×400). (b) Branching and septated hyphae with conidiophores and conidia in basipetal chains seen on lactophenol cotton blue mounts (original magnification ×400).
Treatment with itraconazole (200 mg daily) and terbinafine (250 mg daily) was commenced, but, after one week, the crusted ulcer was much enlarged. We decided to hospitalize the patient, and surgical debridement was performed. Itraconazole and terbinafine administration were simultaneously terminated and intravenous amphotericin B (1 mg/kg daily) was commenced. Approximately 2 weeks later, blood creatinine level increased, but the glomerular filtration rate fell. Amphotericin B therapy was terminated, and itraconazole (200 mg daily) was again administered. During the next 12 weeks, the ulcer size decreased, but repeated fungal cultures revealed growth of the originally isolated organism. Therefore, a flap operation was performed to cover the ulcer, and, simultaneously, drug therapy was changed to itraconazole 125 mg daily and terbinafine 250 mg daily. After 2 weeks, however, our patient reported a palpable nodule on her left temple. A skin biopsy revealed multiple fungal hyphae. She was hospitalized once more and voriconazole (4 mg/kg twice daily) was initiated. However, within one week, blood levels of aspartate aminotransferase and alanine aminotransferase were markedly increased and the drugs were discontinued. We then treated the patient with terbinafine (250 mg daily) and clarithromycin (500 mg twice daily) for 3 weeks. She did not present to us again.
In vitro testing of S. brevicaulis drug susceptibility was performed (3). The minimal inhibitory concentrations (MICs) for amphotericin B were 8 μg/ml, for fluconazole > 64 μg/ml, for itraconazole > 16 μg/ml, for voriconazole 4 μg/ml, for caspofungin 4 μg/ml, and for micafungin > 16 μg/ml.
DISCUSSION
Although 1–10% of onychomycosis cases are caused by S. brevicaulis, cutaneous infections are rare (except in the nails) (1). In immunocompetent patients, S. brevicaulis infections usually develop after trauma or surgery. However, cutaneous S. brevicaulis infections without previous injury have been reported (4–7). In immunocompromised patients, several cases of invasive systemic infections have been reported (8–10).
Treatment of S. brevicaulis infections is difficult. Several drug susceptibility studies have shown that the organism is resistant to broad-spectrum antifungal agents including amphotericin B, flucytosine, fluconazole, itraconazole, voriconazole, and terbinafine (7, 11, 12). However, in many cases, in vitro data differ from in vivo observations (5, 6). Generally, in immunocompetent patients, cutaneous S. brevicaulis infections can be treated successfully using modern antifungal agents. However, the minimal fungicidal concentration (MFC) for S. brevicaulis is higher than the MFC for dermatophytic fungi. In a previous report of cutaneous S. brevicaulis infection, ringworm lesions on the legs of a 14-year-old girl were cleared with terbinafine (250 mg daily) and itraconazole (100 mg daily) (4). An ulcerative granulomatous cheilitis with lymphatic invasion in a 43-year-old man was completely healed on administration of itraconazole (200 mg daily) for 2 months (5). In that case, the itraconazole MIC for S. brevicaulis was greater than 100 μg/ml (5). However, a plantar infection in a 42-year-old woman was resistant to both terbinafine and itraconazole (6). In addition, a granulomatous skin infection in a 14-year-old girl could not be readily cleared with terbinafine and itraconazole (7). In immunocompromised patients, treatment tends to be much more difficult.
Therefore, some authors have recommended a combination of surgical debridement and antifungal agent therapy to clear S. brevicaulis infections (8, 9). In our patient, however, several combination treatments, including itraconazole, terbinafine, amphotericin B, and voriconazole, with concurrent surgical debridement, failed to resolve the problem.
A similar case has been reported in a Korean journal (13). A 54-year-old woman, who had received filler injections, developed cellulitis-like lesions. Liposuction was performed to remove foreign materials and necrotic tissue, and pus cultures revealed S. brevicaulis infection. Although this patient did not ingest any antifungal agents, no recurrence was noted at 6 months. In another interesting case, antifungal- and cryotherapy-resistant subcutaneous hyalohyphomycosis in an immunocompetent patient was almost completely healed within one month after application of topical 5% imiquimod cream (14). Although the causative fungus, Acremonium strictum, was not the same as in our patient, the observation may be relevant.
Our patient received a collagen injection from an unlicensed practitioner. We have treated one other patient with a Mycobacterium chelonae infection developed after collagen injection by the same person (15).
REFERENCES