A Crescent-shaped Nodule in the Temple: A Quiz
Woon-Kyong Chung1, Gyeong-Hun Park1, Seong-Min Kang1, Ho-Seok Suh2, Mi-Woo Lee1*, Jee-Ho Choi1, Kee-Chan Moon1
Department of Dermatology, University of Ulsan College of Medicine, 1Asan Medical Center, 388-1 Pungnap-dong, Songpa-gu, 138-736 Seoul, 2Ulsan University Hospital, Ulsan, Korea. E-mail: 1052_hihi@hanmail.net
A 32-year-old Korean woman presented to our clinic with a solitary crescent-shaped protruding nodule on the right temporal area (Fig. 1). Approximately one year previously, a single tiny papule that had not been associated with trauma had suddenly increased in size to a 2 × 1 cm, protruding, crescent-shaped nodule. At that time, the patient was pregnant and refused treatment; however, she returned to the clinic after giving birth. In the intervening period, the size and shape of the nodule had not changed.
Fig. 1. Solitary crescent-shaped protruding nodule in the right temporal area.
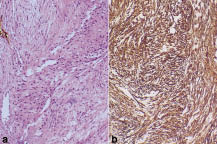
Histopathological examination showed a poorly circumscribed mass in the lower dermis, and subcutaneous fat, infiltrating into the muscular structure (Fig. 2a). Cellular atypia was not prominent. Abundant fibrous tissue and mild infiltration of inflammatory cells were also noted. Dermal collagen bundles were densely packed. Immunohistochemical analysis showed that spindle-shaped cells were positive for smooth muscle actin (Fig. 2b), but negative for CD34, CD31, factor XIII and factor VIII.
Fig. 2. Histologic examination revealed spindle-shaped plump cells deposited in the myxoid stroma (a). Immunohistochemical analysis showed that the cells were positive for smooth muscle actin (b).
What is your diagnosis? See next page for answer.
doi: 10.2340/00015555-0735
A Crescent-shaped Nodule in the Temple: Comment
Acta Derm Venereol 2009; 89: 668–671 (contd).
Diagnosis: Nodular fasciitis
Nodular fasciitis (NF) was first reported as subcutaneous pseudosarcomatous fibromatosis by Konwaler et al. in 1955 (1). The term “pseudosarcomatous” was chosen owing to its rapid growth, high cellularity, frequent mitoses and infiltrative border.
Clinically, NF usually occurs in young adults as a subcutaneous or deep soft-tissue mass and grows rapidly (2, 3). Although the extremities are most commonly involved, it is estimated that 10–20% of cases involve the head and neck region (1, 3).
Most cases of intradermal fasciitis occur in the head and neck region (4, 5). Meffert et al. (6) highlighted that in the head and neck region, the fascial musculature is directly attached to relatively thin skin through the superficial musculoaponeurotic system. The temporal area is the region of the face with the thinnest skin; therefore, rapid growth of NF in this area may raise the skin.
NF on the face should be differentiated from facial dermatofibroma, dermatofibrosarcoma protuberance, or atypical fibroxanthoma. Histopathological features, such as the fibrillar character of tumour cells with smooth muscle actin, and abundant dermal mucin might be diagnostic indicators of NF.
NF follows a self-limiting course and recurrence is uncommon; hence a wide excision should be avoided.
REFERENCES