Emilie Imbert1, Brigitte Milpied1, Thomas Jouary1, Julie Versapuech1, Jean-François Goussot2, Alain Taieb1 and Khaled Ezzedine1
1Department of Dermatology, CHU Saint-André, 1, rue Jean Burguet, FR-33075 Bordeaux, and 2Department of Pathology, CHU Haut-Lévêque, Pessac, France. E-mail: khaled.ezzedine@chu-bordeaux.fr
Accepted June 30, 2009.
Sir,
Paraffinoma is a rare condition that occurs following the injection of mineral oil into subcutaneous tissues. The histology of the condition is that of foreign-body reaction. The technique has been used largely for cosmetic purposes and penile enlargement since early in the 20th century.
Case report
A 40-year-old circumcised heterosexual Caucasian man, originating from Bulgaria and living in France for the last 2 years presented with a one-month history of penile swelling associated with a painful ulceration. Past medical history was unremarkable and the patient denied any at-risk sexual behaviour. Physical examination revealed painful oedematous ulcerated penile involvement. The lesion was clean with fibrin deposit and there was neither palpable inguinal lymph node nor urethral discharge. Laboratory evaluations were within normal limits. Bacteriological and viral swabs from the ulceration, as well as serodiagnostics for trepanomatoses, and human immunodeficiency, hepatitis B and C viruses, were performed and failed to reveal any infectious involvement. A skin biopsy specimen obtained from the indurated border of the ulcer was stained with haematoxylin-eosin and periodic acid-Schiff.
Fig. 1. Painful swelling and ulceration of the penis in a 40-year-old Caucasian male.
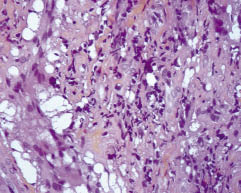
Histopathological examination revealed marked thickening of the reticular dermis with aggregates of vacuoles of varying size, often surrounded by multinucleated giant cells. There was dense sclerosis of the intervening stroma and a patchy lymphoid infiltrate. Polarization examination was negative.Based on this, a diagnosis of paraffinoma was made. Although the patient first denied injection of mineral oil into the penis, he further acknowledge the causative practice.
Fig. 2. Marked thickening of the reticular dermis with aggregates of vacuoles of varying size, often surrounded by multinucleated giant cells (H&E × 300).
The patient declined any surgical intervention, and treatments including intralesional injection of triamcinolone acetonide (one injection per month for a total of 3 months) and the topical application of hydrocolloid gel for the ulceration were commenced. Four months later, oedema had partially resolved and the ulcerations had completely healed, leading to small depressed atrophic lesions.
DISCUSSION
Paraffinoma, also known as mineral oil granuloma, is the term used to describe an unusual histopathological pattern showing the substitution of normal subcutaneous tissues by cystic structures of various size. Paraffinomas have been encountered with the injection of numerous oily foreign substances that contain straight-chain saturated hydrocarbons. Because of the inability of human enzymes to degrade these substances, a granulomatous foreign-body reaction may occur. Mineral oils have been widely used for cosmetic purposes and, in European Eastern countries and Korea, they are still used for penis enlargement (1–3). Of note, patients are often unwilling to admit to the practice. The lesions are known to have lag times from weeks to several years after the provocative injections, as was the case in our patient (4). Differential diagnosis, especially when fistulization and ulceration are present, should include venereal disease. Moreover, inflammation associated with mineral-oil injections may trigger squamous cell carcinoma as has been reported previously, and patients should be screened in case of wide ulcers with cyclic borders (5, 6). Although some authors have reported successful treatment with potent topical corticosteroids, the treatment of choice for paraffinoma remains a complete surgical excision, otherwise recurrence of symptoms is common (7).
Public awareness is required for the prevention of physically and psychologically disturbing sequelae resulting from penile injections. With respect to penile enlargement in patients with low self-esteem and sexual and relational dysfunction, several surgical techniques, including injections of autologous fat, grafts of dermal-fat strips, as well as release of suspensory ligaments are currently under investigation (8, 9). Although paraffinomas are not common, physicians should be aware of this entity, keeping in mind the unwillingness of patients to admit to this practice.
References