Natsuki Kuraishi, Yayoi Nagai, Michiko Hasegawa and Osamu Ishikawa
Department of Dermatology, Gunma University Graduate School of Medicine, Gunma, Japan



Natsuki Kuraishi, Yayoi Nagai, Michiko Hasegawa and Osamu Ishikawa
Department of Dermatology, Gunma University Graduate School of Medicine, Gunma, Japan
Cutaneous adverse effects of imatinib mesylate (Glivec®) are common and various types of skin eruptions have been reported. We report here a 57-year-old man who presented with lichen planus-like lesions on his extremities and palmoplantar hyperkeratosis due to the use of imatinib mesylate for chronic myeloid leukaemia. The skin lesions improved after discontinuation of imatinib mesylate but re-administration of the drug at a lower dose provoked a mild recurrence. He could, however, continue to take the drug at the lower dose and his skin lesions were well-controlled by topical corticosteroid treatment. The literature on lichenoid drug eruption due to imatinib mesylate is reviewed. Key words: lichenoid drug eruption; palmoplantar hyperkeratosis; imatinib mesylate.
(Accepted August 17, 2009.)
Acta Derm Venereol 2010; 90: 73–76.
Natsuki Kuraishi, Department of Dermatology, Gunma University Graduate School of Medicine, 3-39-22, Showamachi, Maebashishi, Gunma 371-8511, Japan. E-mail: natsukik@showa.gunma-u.ac.jp
Imatinib mesylate can cause several types of adverse effects. There have been reports of several cases of lichenoid eruption on the skin or oral mucosa (1–8); however, palmoplantar hyperkeratosis has rarely been described (9). We report here a patient who developed both lichenoid eruption on the extremities and palmoplantar keratosis due to imatinib mesylate for chronic myeloid leukaemia (CML).
CASE REPORT
A 57-year-old man with CML began treatment with imatinib mesylate in September 2006. He noticed a pruritic eruption 2 months later. At that time, discontinuation of imatinib mesylate along the administration of oral antihistamine agents and topical corticosteroids improved his skin lesions. Because of the worsening of his CML, imatinib mesylate, 400 mg/day, was restarted and the skin eruption exacerbated. He was referred to our department in April 2007.
Physical examination revealed slightly elevated violaceous erythemas with white streaks and scales on his forearms and the dorsal side of his lower legs (Fig. 1). On the dorsal side of his fingers and hands, keratotic erythemas were noted. On his palms and soles, keratotic erythemas with scales were prominent (Fig. 2). A skin biopsy from the violaceous erythema of the forearm was performed under the suspected diagnosis of lichenoid eruption due to imatinib mesylate. Histological examination revealed hyperkeratosis, acanthosis and band-like cellular infiltration with dilated small vessels in the upper dermis (Fig. 3a). Liquefaction degeneration and lymphocyte infiltration into the epidermis was obvious. Civatte bodies were present in the epidermis and dermis (Fig. 3b). A direct immunofluorescence test revealed deposition of IgG, IgM, IgA and C3 at the Civatte bodies.
Fig. 1. Purple reddish, slightly elevated erythemas and nodules with scales on the dorsal side of the lower legs.


Fig. 2. Keratotic erythemas with scales on the palms.
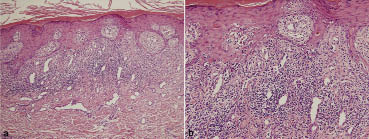
Fig. 3. (a) Histological examination of the forearm revealed hyperkeratosis, acanthosis and band-like cellular infiltration with dilated small vessels in the upper dermis. (b) Higher magnification showed liquefaction degeneration. Civatte bodies were seen in the epidermis and dermis. a) H&E × 100, b) H&E × 200.
As imatinib mesylate had been discontinued one week before his first visit to our hospital, treatment with an oral antihistamine agent and a topical corticosteroid was started. His skin symptoms improved, but did not disappear. Six months after the initiation of treatment with interferon for CML, imatinib mesylate was re-administered at a lower dose of 100 mg/day. Mild keratotic erythemas recurred on his palms and new lesions developed on his buccal mucosa. However, he could continue to take imatinib mesylate along with the antihistamine agent and topical corticosteroid.
DISCUSSION
Imatinib mesylate is a molecularly-specific oral anticancer agent that selectively inhibits several protein tyrosine kinases central to the pathogenesis of human cancer (10). It has been approved in the USA as the first-line therapy for CML and gastrointestinal stromal tumour and has also been introduced for the treatment of metastatic dermatofibrosarcoma protuberans, hypereosinophilic syndrome and other myeloproliferative disorders (11). Recently, the efficacy for systemic sclerosis (12, 13) and nephrogenic systemic fibrosis (14) has also been reported.
Most adverse reactions of imatinib mesylate are mild to moderate and include nausea, oedema, myalgia, diarrhoea and cutaneous reactions. Approximately 31–44% of patients who took imatinib mesylate experienced cutaneous reactions (15). In general, the incidence and severities of adverse effects tend to depend on the dosage of imatinib mesylate. The most common skin rash is a maculopapular type affecting the forearms and trunk. Other cutaneous reactions include hair repigmentation or hypopigmentation, morbilliform eruption, pruritus and lichenoid eruption (10). Severe cases with acute generalized exanthematous pustulosis (AGEP) and Stevens-Johnson syndrome have also been reported (11).
Lichenoid reaction due to imatinib mesylate may be mild to extensive. Fourteen patients, including our case, are summarized in Table I (1–8). Three patients had only mucosal lesions, six had only cutaneous lesions and five had both lesions. Most of the patients took imatinib mesylate, 400 mg/day, and the length of time before the adverse effects appeared after the initiation of the drug ranged from one month to 6 months. In two patients, a systemic corticosteroid was required to improve the skin symptoms. Ten patients could continue or restart treatment with imatinib mesylate. Dalmau et al. (6) reported a patient whose skin lesion was successfully treated with acitretin , enabling the continuation of the effective imatinib mesylate dosage. In our patient, a dose reduction was required to continue imatinib mesylate after temporary discontinuation.
Table I. Cases of lichenoid drug eruption due to imatinib mesylate
| No. | Author, year (ref) | Age (years)/sex | Disease | Dose of imatinib mesylate (mg) | Duration (months)a | Skin eruption | Mucosal lesions | Other treatments | Imatinib treatment |
| 1 | Lim & Muir, 2002 (1) | 72/F | CML | ND | 5 | (–)b | Erosion of the tongue |
| Discontinued |
| 2 | Roux et al., 2004 (2) | 52/M | CML | 400 | 2 | Disseminated eruption | (–) |
| Tentative discontinuation |
| 3 | Ena et al., 2004 (3) | 62/M | GIST | ND | 12 | (–) | Grey-violaceous plaques on the cheeks | Oral corticosteroids | Continued |
| 4 | Prabhash & Dovel, 2005 (4) | 50/M | CML | 400 | 6 | Maculopapular lesions on the eyelids | (–) |
| Continued |
| 5 | Pascual et al., 2006 (5) | 69/F | CML | 400 | 2 | Pruritic papules and plaques | (–) |
| Tentative discontinuation |
| 6 | Pascual et al., 2006 (5) | 65/F | CML | 400 | 3 | Grey violaceous plaques on the trunk | Disseminated violaceous erythemas on the trunk | Oral and topical corticosteroids | Continued |
| 7 | Dalmau et al., 2006 (6) | 76/M | CML | 400 | 4 | Erythema and lichenoid rash on the trunk and upper limbsc | (–) |
| Discontinued |
| 8 | Dalmau et al., 2006 (6) | 60/M | CML | 400 | 2 | Lichenoid eruption on the face, wrist and neck | Reddish macules and erosion | Oral corticosteroids | ND |
| 9 | Dalmau et al., 2006 (6) | 75/M | GIST | 400 | 1 | Generalized eruption | (–) | Acitretin 25 mg/day was effective | Continued |
| 10 | Dalmau et al., 2006 (6) | 50/M | CML | 400 | 2 | Generalized eruption on the face, chest and extremities | White reticulate macules on the buccal mucosa | Acitretin 25 mg/day was effective | Continued |
| 11 | Basso et al., 2009 (7) | 85/? | CML | 400 | ND | Skin eruption on the extremities | Ulcer on the lower lip | PSL 40 mg/day | Discontinued |
| 12 | Basso et al., 2009 (7) | 55/M | CML | ND | 3 | (–) | Erosions on the tongue, lower lip and buccal mucosa | Systemic corticosteroid | Continued |
| 13 | Chan et al., 2007 (8) | 56/M | CML | 600 | 3 | Violaceous papules and plaques on the extremities and chest | (–) | PSL 20 mg/day and topical corticosteroid | Tentative discontinuation |
| 14 | Present case | 57/M | CML | 400 | 2 | Lichenoid eruption on the extremities palmoplantar keratosisd | White streak with erosion on the buccal mucosa | Topical corticosteroid | Tentative discontinuation restarted with reduction of the dose |
aFrom the initiation of imatinib.
bImmunofluorescence study was negative.
cSubungal hyperkeratosis of fingernails.
dImmunofluorescence study was positive at Civatte bodies.
ND: not described; CML: chronic myeloid leukaemia; PSL: prednisolone; GIST: gastrointestinal stromal tumour; M: male; F: female.
Our patient presented with palmoplantar hyperkeratosis rather than lichenoid eruptions. Deguchi et al. (9) reported three cases with psoriasiform palmoplantar hyperkeratosis after long-term imatinib mesylate treatment. In two cases, nail dystrophy was also present. In three cases, discontinuation or dose reduction of imatinib mesylate led to the improvement of all lesions. They reported that hyperkeratotic lesions revealed psoriatic findings, but that the mechanism of action was unclear.
Imatinib mesylate inhibits tyrosine kinases of bcr-abl, c-kit and platelet-derived growth factor receptors (PDGFR). PDGFR and c-kit have not been identified in normal keratinocytes, while c-kit was recently found to be expressed by murine epithelial cells. Several lines of evidence show that PDGFR and stem cell factor may be involved in the pathogenesis of psoriasis, suggesting a possible mechanism of action by which imatinib mesylate causes the psoriasiform reaction. The possibility that altered expression of c-kit may induce epidermal inflammation and other changes in epidermal homeostasis merits further investigation (9). Hypopigmentation due to imatinib mesylate may be related to the inhibition of melanocyte c-kit receptor tyrosine kinase (16, 17).
Because of its relatively low molecular weight and the dose dependency of adverse events, imatinib mesylate does not appear to be immunogenic. A gradual increase in the dose may allow us to reinstitute the therapy after the resolution of cutaneous eruptions. The use of a systemic or topical corticosteroid and a gradual increase in the imatinib mesylate dose could be a practical strategy to enable the continuation of treatment with imatinib mesylate without other antineoplastic treatments.
The authors declare no conflict of interest.
REFERENCES

