Gyeong-hun Park, Chae-hwa Kim, Woon-kyong Chung, Chong-hyun Won, Sung-eun Chang, Mi-woo Lee*, Jee-ho Choi and Kee-chan Moon
Department of Dermatology, Asan Medical Center, University of Ulsan College of Medicine, 388–1 Pungnap-2 dong Songpa-gu, Seoul 138–736, Korea. *E-mail: miumiu@amc.seoul.kr
Accepted November 11, 2009.
Intravascular large B-cell lymphoma (IVLBL) is a rare type of non-Hodgkin’s lymphoma characterized by selective growth of neoplastic cells within the vascular lumen (1). IVLBL frequently manifests with cutaneous symptoms of various morphologies and distributions, such as painful indurated erythematous eruption, poorly circumscribed violaceous plaques, cellulitis, large solitary plaques, painful blue-red palpable nodular discolorations, tumours, ulcerated nodules, small red palpable spots, or erythematous desquamative plaques (2). Although IVLBL is generally regarded as a disseminated disease (1), “cutaneous variants” of IVLBL exist; these are limited exclusively to the skin and are classified as primary cutaneous IVLBL by the World Health Organization–European Organization for Research and Treatment of Cancer (WHO–EORTC) (2, 3).
IVLBL is associated with poor prognosis in most patients, but patients with cutaneous variants have better survival (3). Although anthracycline-based chemotherapy has been the cornerstone of IVLBL treatment (4), no standard treatment guidelines have yet been established (5). Recently, rituximab-containing chemotherapies have appeared promising (4, 6, 7), but neither the efficacy nor safety of such chemotherapies has been sufficiently evaluated, especially in treatment of cutaneous variants.
CASE REPORT
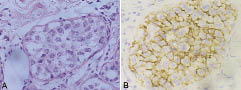
A 62-year-old woman presented with a 4-month history of multiple violaceous scaly tender patches on both lower legs (Fig. 1 A, B). She had no fever, weight loss, or night sweating. A biopsy from the right lower leg lesion showed numerous atypical large cells with irregular nuclear contours and prominent nucleoli clustered in dilated dermal blood vessel lumens (Fig. 2A). These cells stained positive for CD20 (Fig. 2B) and CD79a, but negative for CD3, CD4, CD8, CD30, CD56, and cytokeratin. Based on these findings, the skin lesions were diagnosed as IVLBL.
Fig. 1. Multiple violaceous scaly patches on the medial aspects of (A) the right and (B) the left lower legs. (C) Multiple hypermetabolic lesions in the anterior, medial and lateral cutaneous and subcutaneous areas of both lower legs revealed by positron emission tomography scan.
Fig. 2. (A) Numerous atypical large cells with irregular nuclear contours and prominent nucleoli clustered in the dilated dermal blood vessel lumens (haematoxylin and eosin stain; ×400). (B) Immunohistochemical staining of tumour cells showing CD20 positivity (×400).
Laboratory data indicated a low white blood cell count of 3.7 × 103/mm3 (normal 4.0–10.0 × 103/mm3), a low haemoglobin level of 10.2 g/dl (normal 12.0–16.0 g/dl) and a platelet count of 182 × 103/mm3 (normal 150–350 × 103/mm3), an elevated serum lactate dehydrogenase level of 280 IU/l (normal 120–250 IU/l), and a normal uric acid level of 3.2 mg/dl. No additional lymphoma lesion was found by computed tomography (CT) of the chest, abdomen, and pelvis, magnetic resonance imaging (MRI) of the brain, whole-body positron emission tomography (PET) scan (Fig. 1C), or bone-marrow biopsy.
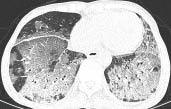
The patient received three cycles of rituximab (375 mg/m2) and CHOP (cyclophosphamide 750 mg/m2 on day 1, doxorubicin 50 mg/m2 on day 1, vincristine 2 mg on day 1, and prednisolone 100 mg on days 1–5), with each cycle lasting for 3 weeks. After the first cycle, the skin lesions improved markedly and pain and tenderness disappeared. At completion of the third cycle, a whole-body PET scan showed complete metabolic responses in the cutaneous and subcutaneous layers of both lower legs, but disclosed newly developed diffuse ill-defined hypermetabolic lesions in both lung fields, suggestive of drug-related inflammatory changes. Although the patient complained of mild dyspnoea, there was no active lesion on chest radiography. The fourth cycle was begun as scheduled with CHOP, excluding rituximab, but 15 days after commencement the patient was admitted to hospital because of high fever, dry cough, and chest discomfort. High-resolution computed tomography (HRCT) of the chest revealed newly developed diffuse ground-glass opacity in both lungs with peripheral dominancy in both upper lobes and a scanty effusion in the left hemithorax (Fig. 3). The bronchoalveolar lavage fluid was negative for bacteria, acid-fast bacilli, respiratory syncytial virus, influenza virus, parainfluenza virus, adenovirus, cytomegalovirus, and Pneumocystis carinii. Transbronchial lung biopsy results showed alveolar pneumocyte hyperplasia with intra-alveolar hyaline membranes. After intravenous methylprednisolone (2 mg/kg/day) was initiated, body temperature became normal within one day and chest radiography showed slow lung improvement. Six weeks after discharge, additional two cycles of CHOP without rituximab were given, with 30% dose reductions of cyclophosphamide and doxorubicin, at intervals of 3 weeks.
Fig. 3. High-resolution computed tomography of the chest demonstrating diffuse ground-glass opacity in both lungs 2 weeks after the start of the fourth cycle of CHOP (cyclophosphamide, doxorubicin, vincristine, prednisolone).
A skin biopsy from the right lower leg 6 months later revealed no evidence of lymphoma. There was scanty lymphocytic cell infiltration, and the cells stained positive for CD3, CD20, and CD79a. Complete metabolic response was repeatedly shown on whole-body PET scans performed 3, 9 and 15 months after treatment. No recurrence has been observed in the 19 months since complete metabolic response was achieved.
DISCUSSION
The cutaneous variant of IVLBL is rarer in Asia (3% of IVLBL patients) than in Western countries (24%) (1), and only one patient with IVLBL featuring cutaneous involvement has been reported in Korea (8). Patients with the “cutaneous variant” are mostly females of younger age with normal leukocyte and platelet counts (2). Most patients with single lesions enjoy long-term survival, and prolonged remission can sometimes be achieved by application of local strategies. However, most patients with multiple lesions relapse within one year of treatment notwithstanding the use of systemic anthracycline-based chemotherapy (2).
Rituximab is a genetically engineered monoclonal antibody consisting of the variable region of a murine anti-CD20 antibody and the constant regions of human IgG1 heavy and light chains (9). The addition of rituximab to the CHOP regimen improves outcomes in patients with newly diagnosed diffuse large B-cell lymphoma (10), and rituximab-CHOP with or without field radiotherapy is recommended as the first-line treatment for primary cutaneous diffuse large B-cell lymphoma, leg type (11). Recently, outcomes of IVLBL patients who received chemotherapy either with or without rituximab were analysed (4, 6, 7). Complete response rates and survival outcomes were significantly higher in the rituximab-treated groups (4, 7). However, the outcomes of patients with cutaneous disease variants were not separately described.
Rituximab-induced interstitial lung disease is very rare, but can be fatal (12, 13). Patients with this condition are usually elderly and present with dyspnoea, dry cough, hypoxemia, and occasionally fever (12). HRCT of the lung shows diffuse interstitial patterns, and a lung biopsy can demonstrate interstitial inflammation or fibrosis (12, 13). The mechanism of this lung injury remains unclear (12). Reported underlying diseases include chronic lymphocytic leukaemia, diffuse large B-cell lymphoma, mantle cell lymphoma, immune thrombocytopenic purpura, and extranodal marginal zone B cell lymphoma (13, 14). However, no report of rituximab-induced interstitial lung disease arising from IVLBL has appeared in the literature.
In summary, we report here a patient with primary cutaneous IVLBL treated with rituximab-CHOP and complicated by rituximab-induced interstitial lung disease successfully treated with intravenous corticosteroids.
REFERENCES