Psoriasis is a chronic skin disease associated with problems in body image and self-esteem and feelings of stigma and shame. The aim of this study was to analyse the clinical extent of psoriasis and its association with psychological distress, and to compare the psychopathological traits in early-onset (type I: age of onset < 40 years) vs. late-onset (type II: age of onset > 40 years) psoriasis. A total of 140 patients participated in the study; 70 patients with confirmed diagnosis of psoriasis vulgaris and 70 patients as a comparative group. A battery of psychological instruments was used together with an Inventory of life stress events. The severity of psoriasis was assessed by standardized Psoriasis Area and Severity Index measure. The Psoriasis Life Stress Inventory showed the significant correlation with clinical extent of psoriasis and other measures of psychological distress. Patients with late-onset psoriasis had more prominent symptoms of depression compared with the group with early-onset psoriasis and the comparative group. The results of the Minnesota Multiphasic Personality Inventory-201 for the patient group with late-onset psoriasis showed a specific configuration of neurotic triad. Key words: psoriasis; depression; anxiety; stress; psychopathological traits.
(Accepted December 3, 2009.)
Acta Derm Venereol 2010; 90: 251–256.
Lena Kotrulja, University Department of Dermatology and Venereology, Sestre milosrdnice University Hospital, Vinogradska 29, 10000 Zagreb, Croatia. E-mail: lena.kotrulja@zg.t-com.hr
Psoriasis is a chronic, genetically influenced and immunologically based inflammatory disease of the skin (1) that affects approximately 1.5–3% of the population. It is important for clinicians to be aware that psoriasis can have a substantial emotional impact on the individual, which is not necessarily related to the extent of the skin disease (2). It has long been recognized that living with a chronic condition, such as psoriasis, can have a considerable impact on the individual concerned. In turn, there is an increased understanding that psychological distress encountered as a result of this experience can have implications for the course of the disease (3). The role of stress in the onset of, and as a trigger for, exacerbation of psoriasis has been debated for many years. Life stresses have been ascribed as both a cause of psoriasis and as an aggravating factor in the disease (4, 5). Psoriasis is associated with a variety of psychological problems, including poor self-esteem, sexual dysfunction, anxiety, depression and suicidal ideation. The clinical severity of psoriasis may not reflect the degree of emotional impact of the disease (2). It has been observed that two clinical forms of psoriasis can be distinguished: type I, with an early age onset (< 40 years); and type II, with late age onset (> 40 years) (6). Psoriasis of early onset has been associated with a greater genetic susceptibility and a more severe and recurrent course, while psoriasis of late onset has no determined genetic component and is therefore considered to be more reactive, i.e. susceptible to environmental factors (6–8).
The aim of the present study was to explore, in a group of patients with psoriasis, the relationship between measures of clinical status (Psoriasis Area and Severity Index; PASI) and various measures of psychological status, in order to examine the relationship between the psychosocial aspects of psoriasis and the extent of the disease. A further aim was to test the hypothesis that certain psychopathological traits, which render the patient more susceptible to environmental factors such as stress, would be more frequently associated with late-onset than early-onset psoriasis.
MATERIALS AND METHODS
Patients
The study was carried out on a convenience sample comprising 140 patients (67 men and 73 women, age range 23–82 years; mean 49.8, SD 15.1): 70 patients with confirmed diagnosis of psoriasis vulgaris (by dermatological clinical assessment and histological verification, 44 of them with type I and 26 with type II) and 70 patients considered as a comparative group (patients with other dermatoses not perceived as psychosomatic; from which 9 patients diagnosed as contact allergic dermatitis, 13 patients with diagnosis of contact irritant dermatitis, 10 patients diagnosed as basocellular carcinoma, 2 patients with squamous cell carcinoma, 7 patients with dysplastic naevi syndrome, 15 patients with onychomycosis, 5 patients with onychodystrophy and 9 with dermatomycosis). The distribution of patients according to age and sex is presented in Table I. There was no statistically significant difference in sex among three groups of patients (χ2 = 4.84, p > 0.05), while the age difference was statistically significant (F(2,137) = 20.28, p < 0.05). The patients were examined at the Department of Dermatology and Venereology of Sestre milosrdnice University Hospital and University Hospital Centre and School of Medicine, Zagreb, Croatia. Patients were excluded if they were under 18 years of age, had any severe mental or physical illness and did not have a diagnosis of psoriasis confirmed by a dermatologist (including histological confirmation). All eligible patients who gave their written informed consent were recruited in the study. Ethical approval was granted by the Institutional Review Board and the study was carried out in compliance with the Declaration of Helsinki guidelines. Psoriatic patients were evaluated by a dermatologist who collected sociodemographic data (age, sex, education, employment and marital status) and history of the disease (age of onset, duration, extension of the disease, heritability), and assessed the clinical severity of psoriasis. The patients also completed a battery of psychological questionnaires under the supervision of a psychologist.
Table I. Age and sex distribution of three groups of patients
| | Mean age (years) |
| Psoriasis type I n = 44 | Psoriasis type II n = 26 | Comparative group n = 70 |
| Male | 41.3 (n = 25) | 60.9 (n = 15) | 53.7 (n = 27) |
| Female | 43.0 (n = 19) | 66.0 (n = 11) | 47.2 (n = 43) |
Instruments
Clinical severity instrument. The dermatological status/clinical severity of psoriasis was assessed by a dermatologist using the PASI (9). Points for erythema, infiltration and desquamation of the skin ranged from 1 to 4, and the involved area from 1 to 6, thus, theoretically the PASI ranges from 0 to 72, with higher scores indicating more severe condition. PASI less than 3 was scored as score 1 (or mild), PASI ≥ 3 and < 15 as score 2 (or moderate), and PASI ≥ 15 as score 3 (or severe) (9–11).
Specific and generic measures of psychological distress. We used a variety of psychological instruments to screen for the broad range of psychopathological factors that have been implicated in psoriasis. The psychological instruments were as follows:
- General Health Questionnaire (GHQ), a 28-item self-administered questionnaire measuring the probability of a minor psychiatric disorder (or amount of psychological distress), covering the symptoms of anxiety, depression, self-esteem and day-to-day difficulties. The instrument is scored from 0 to 28, with higher scores indicating greater psychological distress. A score of 0–3 points indicates a normal level of mental well-being, a score of 4–6 points indicates mild distress, while the score ≥ 6 points to a higher level of psychological distress (12).
- A 21-item version of Beck Depression Inventory (BDI) for measuring depression (13). Responses were scored on a scale from 0 to 63, with higher scores indicating greater depression. A score of 10 points was established as a cut-off point for assessing mild depression, and the score higher than 24 indicated a clinically manifest depression (14).
- State-Trait Anxiety Inventory (STAI) comprises two separate self-report scales for measuring two distinct anxiety concepts: state anxiety (A-State) and trait anxiety (A-Trait). The STAI A-Trait scale consists of 20 statements and the participants have to assess “how they generally feel”. The A-State scale consists of 20 statements with questions about “how they feel at a particular moment in time”. The A-Trait scale is used as a research tool for selecting subjects who vary in their disposition to respond to psychological stress and A-State scale is used to determine the actual/transitory level of anxiety induced by stressful life events. The range of possible scores for STAI varies from a minimum score of 20 to a maximum score of 80 on both the A-State and A-Trait subscales, with higher score indicating higher level of anxiety (15, 16).
- Psoriasis Life Stress Inventory (PLSI) – the 15-item version PLSI was developed to measure psoriasis-related stress and represents an index of the psychosocial morbidity associated with psoriasis (17). Subsequent research has shown that the PLSI addresses specifically to a stress resulting from anticipation of other people’s possible reactions leading to avoidance of worrying situations (e.g. “not going to public places when you would have liked to”) and stress resulting from patients’ actual experience of beliefs of being evaluated by others solely on the basis of their skin condition (e.g. “people make a conscious effort not to touch you”) (18). For each item the patient was asked to rate the level of stress experienced over the previous month on a 4-point scale, from “not at all” to “a great deal”. The PLSI score was calculated by summing the scores for each question. The total stress score could range from 0 to 45 and was cut at a value of 10; the patients with score less than 10 were classified as having “low” PLSI scores (i.e. who are not significantly affected by psoriasis-related stress) in comparison with those with scores ≥ 10, who were classified as having “high” PLSI scores (i.e. who react significantly to the stress associated with having psoriasis) (17).
- Minnesota Multiphasic Personality Inventory (MMPI) (19) is one of the most frequently used personality tests. The inventory is used by trained professionals to assist in identifying personality structure and psychopathology. MMPI-201 is a variant of MMPI standardized to the population of former Yugoslavia (20). It consists of 201 statements, which can be rated by the patient as “correct” or “incorrect.” Statements are grouped into 11 scales, and answers may be indicative of one or more of them. Three scales – L, F and K – are the validity scales, measuring the appropriateness and readiness of respondents for this type of testing (response bias): the L scale (also known as ”lie scale”) reflects the rigidity or naiveté in respondents’ approach to the test material; the F scale (”infrequency”) shows confused thinking, lack of understanding of the material, or malingering; and the K scale (”corrections”) reveals a lack of readiness to express one’s own characteristics and a tendency to provide socially acceptable answers. The remaining scales are the clinical scales: Hs (hypochondriasis) scale – narcissism of the body and hypochondriasis; D (depression) scale – depressive symptoms; Hy (hysteria) scale – conversive symptoms; Pd (psychopathic deviation) scale – immaturity, impulsiveness, and asocial behaviour; Pa (paranoia) scale – sensitivity, hostility; Pt (psychasthenia) scale – anxiety and obsessive thinking; Sc (schizophrenia) scale – confused and bizarre thinking; and Ma (hypomania) scale – euphoria and hyperactivity (20, 21). Given that the scales are psychometrically and phenomenologically interconnected, the interpretation of results is based on a profile configuration rather than on an individual scale result. A general rule is that only the scales with T score ≥ 70 (cut-off result) are interpreted. Biro & Berger (20) reported the MMPI-201 to have good metric characteristics. The discriminative and predictive power of the items was increased in comparison with the original scale, while the validity of both the bimodal code, when the final result is based on two most prominent scales, and the entire profile is excellent (19, 20).
- Inventory of stress life events (author’s inventory), analysing the subjective perception of stress in seven categories of potential stress events in everyday life (family, work/school, financial difficulties, hormonal changes, illness/trauma, war experience, other). For each category of stress situations the patient was asked to name the specific situation within the category and rate the level of stress experienced on a 5-point Likert scale, from “not at all” to “extremely high”. Two indices were obtained: a total number of stressors experienced and the corresponding perception of their intensity. The patients were also asked to assess the influence of the experienced stress on the onset/exacerbation of psoriasis, on a 4-point scale, from “not at all” to “a great deal”.
Statistical analysis
The results were presented as frequencies, mean ± SD, or proportions. The participants were divided into three groups according to the disease: psoriatic patients were divided into two groups in relation to the age at onset of illness (type I and type II), while the third group consisted of patients with other dermatological diseases not perceived as psychosomatic. We performed t-test, the analysis of variance (ANOVA) with Scheffé post-hoc tests and χ2 test for testing the differences between groups. Correlations between variables were assessed with Pearson’s correlation coefficients. The level of statistical difference was set at p < 0.05.
All statistical analyses were performed under SPSS, version 10.0 for Windows software (22).
RESULTS
Disease severity, onset and duration
In patients with psoriasis type I the mean age of onset of the disease was 25.8 (± 7.2) years, and disease duration was 16.2 (± 9.42) years. In patients with psoriasis type II the mean age of onset was 52.0 (± 8.93) years, and disease duration was 11.0 (± 8.74) years. The difference between groups was statistically significant for both age of onset (t = 13.46, p < 0.05) and duration of disease (t = 2.31, p < 0.05). Clinical severity of the disease measured by PASI showed statistically significant higher scores in patients with type II psoriasis. PASI of 15 or higher was found in 80.8% of patients with type II psoriasis (late onset) compared with 56.8% of patients with type I psoriasis (early onset) (Table II). The total range of PASI scores in patients with type I psoriasis was from 2.4 to 51.9, and for patients with type II psoriasis from 6.4 to 46.2.
Table II. Proportion of patients with type I and type II psoriasis according to the clinical severity Psoriasis Area and Severity Index (PASI) and Psoriasis Life Stress Inventory (PLSI) score
| | Psoriasis type I (%) | Psoriasis type II % |
| PASIa |
| (1) < 3 (mild) | 2.3 | 0 |
| (2) ≥ 3–15 (moderate) | 40.9 | 19.2 |
| (3) > 15 (severe) | 56.8 | 80.8 |
| PLSIb |
| < 10 (mild) | 25.0 | 7.7 |
| > 10 (high) | 75.0 | 92.3 |
aχ2 = 5.05; p < 0.05, bχ2 = 3.23; p > 0.05.
Perceived influence of stress
The PLSI score ranged from 0 to 45. Patients with scores ≥ 10 were classified as having “high” PLSI scores (meaning that they react significantly to the stress associated with having psoriasis).
In the group of psoriatic patients 82.4% had PLSI ≥ 10, meaning that our patients were highly reactive to the stress related to the disease. When comparing patients with early-onset (type I) and late-onset (type II) psoriasis, the difference in the PLSI score was not statistically significant (Table II).
The scores on the Inventory of stress life events enabled us to compare groups of patients in regard to a total number of stressors experienced, the corresponding perception of their intensity and the perception of influence of stress on the onset/exacerbation of the disease. There was no statistically significant difference among groups in the number of stressors (F(2,137) = 2.59, p > 0.05), while the perception of intensity of experienced stress in a group of psoriatic patients was significantly higher than in the comparative group (t = 2.11; p < 0.05). As can be seen from Table III, the majority of patients in comparative group perceive that stress has no influence on their disease, while psoriatic patients, irrespectively of the type of psoriasis, estimate that stress has a major role in exacerbation/onset of their disease.
Table III. Perception of stress influence on exacerbation/onset of disease in psoriatic patients and comparative group
| Estimate of stress influence on disease | Psoriatic patients Type I (%) | Psoriatic patients Type II (%) | Comparative group (%) |
| 1 – not at all | 23.3 | 44.0 | 67.2 |
| 2 – slightly | 25.6 | 12.0 | 9.0 |
| 3 – a lot | 30.2 | 28.0 | 16.4 |
| 4 – a great deal | 20.9 | 16.0 | 7.5 |
χ2 = 21.8; p < 0.05.
Correlation with psychological distress
The comparison of results on specific (BDI, STAI-S, STAI-T) and generic measures (GHQ) of psychological distress among three groups of patients (Table IV) revealed only one significant difference and it was found for the BDI score: patients with type I psoriasis showed no symptoms of depression, while those with type II psoriasis showed symptoms of moderate depression. All three groups showed a state of mild psychological distress (GHQ) and symptoms of mild anxiety, both as a trait and a state (STAI-T, STAI-S).
Table IV. Results of specific and generic measures of psychological distress for three groups of patients
| | Patients with psoriasis type I | | Patients with psoriasis type II | | Comparative group | F | p |
| Mean | SD | | Mean | SD | | Mean | SD |
| General Health Questionnaire | 4.4 | 5.17 | | 5.9 | 6.18 | | 6.0 | 6.59 | 0.97 | > 0.05 |
| Beck Depression Inventory | 8.5a | 5.66 | | 15.4a | 10.72 | | 10.5 | 9.77 | 5.03 | < 0.01 |
| State-Trait Anxiety Inventory – State | 40.4 | 9.16 | | 45.8 | 10.71 | | 42.6 | 11.90 | 1.98 | > 0.05 |
| State-Trait Anxiety Inventory – Trait | 41.4 | 7.70 | | 45.3 | 8.55 | | 41.4 | 9.43 | 2.04 | > 0.05 |
aStatistically significant difference between psoriatic patients type I and type II.
SD: standard deviations; F: analysis of variance (ANOVA) test values.
Pearson’s coefficients of correlation were calculated among PASI score, PLSI score and measures of psychological distress in psoriatic patients. Statistically significant correlations (p < 0.01) were found between PLSI and all the measures of psychological distress (GHQ, BDI, STAI-T and STAI-S), while PASI significantly correlated only with PLSI (p < 0.05) (Table V).Psychopathological characteristic (MMPI-201)
Table V. Pearson coefficients of correlation between clinical severity of psoriasis (Psoriasis Area and Severity Index; PASI), Psoriasis Life Stress Inventory (PLSI) score, and other measures of distress in psoriatic patients
| | PASI | PLSI |
| PASI | – | 0.30a |
| General Health Questionnaire | 0.17 | 0.55b |
| Beck Depression Inventory | 0.11 | 0.59b |
| State-Trait Anxiety Inventory – State | 0.12 | 0.46b |
| State-Trait Anxiety Inventory – Trait | 0.06 | 0.57b |
aCorrelation significant on p < 0.05.
bCorrelation significant on p < 0.01.
Pearson’s coefficients of correlation were calculated between clinical severity (PASI score) and PLSI scores and different MMPI-201 clinical scales in psoriatic patients. Statistically significant correlations were found between PLSI and clinical scales of hypochondriasis, depression, hysteria, paranoia, psychopathic deviation and psychastenia. PASI showed no significant correlations with any of MMPI-201 clinical scales (Table VI).
Table VI. Pearson coefficients of correlation between clinical severity of psoriasis (Psoriasis Area and Severity Index; PASI)), Psoriasis Life Stress Inventory (PLSI) score, and clinical scales of Minnesota Multiphasic Personality Inventory (MMPI-201) in psoriatic patients
| MMPI-201 | PASI | PLSI |
| Hypochondriasis | 0.17 | 0.38b |
| Depression | 0.17 | 0.57b |
| Hysteria | 0.10 | 0.43b |
| Psychopathic deviation | –0.08 | 0.26a |
| Paranoia | 0.03 | 0.35b |
| Psychasthenia | –0.03 | 0.25a |
| Schizophrenia | –0.13 | 0.20 |
| Hypomania | –0.09 | –0.16 |
aCorrelation significant on p < 0.05.
bCorrelation significant of p < 0.01.
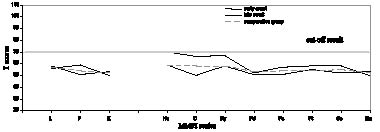
Patients with late-onset type of psoriasis showed the specific psychological profile described as a neurotic triad: elevated D (depression), Hs (hypochondriasis), and Hy (hysteria) scales in the MMPI-201 profile. There was no specific psychological profile in either patients with early-onset psoriasis or the comparative group (Fig. 1).
Fig. 1. Configuration of psychological profile for the group with late-onset (type II) psoriasis showed the specific neurotic triad: (elevated D (depression), Hs (hypochondriasis), and Hy (hysteria) scales) in the Minnesota Multiphasic Personality Inventory (MMPI)-201 profile. L: lie scale; F: infrequency; K: correction; Pd: psychopathic deviation; Pa: paranoia; Pt: psychasthenia; Sc: schizophrenia; Ma: hypomania.
DISCUSSION
Psoriasis is a disfiguring and stigmatizing skin disease, the course of which is punctuated by exacerbations and remissions (2, 23–25). It is associated with problems in body image and self-esteem and feelings of stigma and shame (26). Therefore, the recognition and management of psychological factors have become part of dermatological practice (23, 24). Many psoriatic patients have to deal on a daily basis with shame, guilt, anger and fear of being thought by others as dirty and infectious (27). As the increased levels of stress, anxiety, depression, and anger experienced by patients with psoriasis may be both caused by their condition and exacerbate it (5, 28), it was interesting to compare some of the psychological characteristics in psoriatic patients and comparative group.
However, psoriatic patients cannot be viewed as a homogeneous group. Early-onset psoriasis (type I) has a strong association with HLA-Cw6 as a genetic marker, and has a tendency to become generalized (6, 29), while the late-onset psoriasis (type II) has been reported to be more readily triggered by environmental factors such as stress (8).
Therefore, we decided to divide our patients empirically into two well-defined groups according to age at onset of psoriasis and to compare them both mutually and with a comparative group.
Comparison of PASI scores between the two groups of psoriatic patients revealed that more extensive body surface involvement and higher PASI scores in patients with late-onset psoriasis, contrary to the findings of Ferràndiz et al. (30). The analysis of psychological differences among type I and type II psoriatic patients and the comparative group showed only one significant difference: patients with late-onset psoriasis had more prominent symptoms of depression (BDI score 15.4, indicating a moderate depression) compared with both the group of early-onset psoriasis (BDI score 8.5 – no symptoms of depression) and the comparative group (BDI score 10.5, indicating a mild depression). It is interesting that the depression scores showed a moderate correlation with PLSI, but no significant correlation with PASI, meaning that the severity of psoriasis could not be considered a good predictor for depressive symptoms in these patients. The severity of depression and the increased suicide risk have already been shown not to be always directly correlated with the clinical severity of the dermatological disorder (31).
In the General Health Questionnaire (GHQ) all patient groups achieved scores indicating a mild psychological distress. Both state and trait anxiety scores (STAI-S, STAI-T) indicated the mild anxiety, without differences among groups. We expected our comparative group to show lower levels of psychological distress compared with psoriatic patients, because they were seeking medical help for skin complaints that were trivial in comparison with psoriasis. However, as it has been shown that at least 30% of dermatological patients have some symptoms of psychological distress (23, 24, 31), probably caused by the visibility of their disease, it is not surprising that our very heterogeneous comparative group showed a slight elevation of their scores, comparable to the one usually obtained in patients with various somatic conditions (15).
According to the previous studies, we would expect early-onset psoriasis to be clinically much more severe and extensive, with a greater psychosocial impact than late-onset psoriasis and other dermatological problems (6, 29, 32). However, in our sample the type II psoriasis was both clinically more severe and showed a greater psychological distress. We can only speculate on the causes of type II psoriasis being more severe in our sample. One possible explanation is that the younger patients are more capable of adopting efficient methods for managing the disease, resulting in lessening of their symptoms. As for the difference in psychological variables, we could expect the patients whose disease started at an earlier age to have integrated the physical changes into their self-image. On the other hand, a late onset of the disease, bringing a sudden change in self-image and everyday life, might represent more of a challenge for the self-confidence, and result in feelings of helplessness. This notion is partly supported by the already mentioned higher depression in type II group.
Life stresses have been ascribed as both a cause of psoriasis and as an aggravating factor in the disease (4, 5). As shown in Table III, psoriatic patients perceive stress as the precipitating factor for the onset or exacerbation of the disorder significantly more often than the comparative group.
According to the clinical severity measurements (PASI score), both our groups of psoriatic patients had a very extensive disease, but this almost invariably showed poor correlations with various measures of psychological distress (BDI, STAI-S, STAI-T and GQH), the only exception being PLSI, which correlated significantly with the PASI score (Table V). The finding of no significant correlation between PASI and GHQ, but a significant one between PASI and PLSI, is coincides with the results of Sampogna et al. (33) in a group of 786 psoriatic patients. Previous studies investigating the relationship between clinical variables and quality of life in psoriasis have also found poor correlation, supporting the notion that clinical severity is not a good indicator of subsequent downturn in psychological well-being (18, 34, 35). On the other hand, the PLSI gave us an important insight into the self-perceived daily stress related to the psoriasis and significantly correlated with other measures of psychological distress, and could therefore present a useful screening tool for patients with psoriasis. It should be applied as early as possible during the diagnostic process and psoriatic patients with high score in PLSI should be screened for symptoms of depression and anxiety as well for other symptoms of psychopathology. The evidence of those symptoms would be an indicator for necessity of psychological intervention.
We expected a specific personality profile in patients with psoriasis of late onset, a disease which can be considered as more reactive than type I psoriasis. Indeed, in our study only the former group of patients showed the specific “neurotic triad”. Elevated scores on D (depression), Hs (hypochondriasis), and Hy (hysteria) scales were found in their MMPI-201 profile (20) (Fig. 1). Persons with this profile frequently show psychosomatic reactions, their symptoms resulting from prolonged physiological reactions that naturally accompany negative emotions. Due to suppression or delayed reaction, they can lead to pathological somatic changes (20, 21). Such patients may tend to use maladaptive coping mechanisms and experience excessive autonomic reactivity, when faced with stressful or anger-provoking situations. Although those patients had objectively poorer clinical condition (as measured with PASI), it was not correlated with any of the MMPI scales, while PLSI showed significant correlations with Hs, D, Hy, Pd, Pa and Pt. Our results support the hypothesis about the greater susceptibility of type II psoriasis to exogenous factors, which could be related to the specific psychological profile rendering those patients more vulnerable to environmental stressors.
Clinicians who care for patients with psoriasis need to be mindful of its invisible burdens, including depression and other forms of psychological distress. By applying simple and relatively short screening tools it is possible to identify those patients who would mostly benefit from a timely psychological intervention. As our results show the late-onset psoriasis patients to be more prone to various forms of distress, specific attention should be paid to their psychological well-being.
ACKNOWLEDGEMENTS
We wish to thank the Department of Dermatology and Venereology of Sestre milosrdnice University Hospital and University Hospital Centre and School of Medicine, Zagreb for allowing us to conduct this study, and all the patients who took part in this study.
REFFERENCES