Husein Husein-ElAhmed1, José Aneiros-Fernández2, Salvador Arias-Santiago1, Jose Anerios-Cachaza2 and Ramón Naranjo-Sintes1
Departments of 1Dermatology and 2Anatomopathology, Hospital Universitario San Cecilio, Avda Dr Oloriz s/n, ES-18012 Granada, Spain. E-mail: vhuseinelahmed@hotmail.com
Accepted January 26, 2010.
Alendronic acid is an oral bisphosphonate licensed for prevention and treatment of postmenopausal osteoporosis. We describe here a case of lichenoid dermatosis induced by alendronate.
CASE REPORT
A 72-year-old man with L5 vertebral fracture due to severe osteoporosis had been treated with alendronate 70 mg per week for 2 months. He was referred to our clinic with itchy maculopapular skin lesions on his trunk, palms and soles (Fig. 1). He had history of arthrosis, which was controlled with paracetamol. There were no other drugs in his medical history.
Fig. 1. Lichenoid skin eruption on the trunk showing maculopapular itchy lesions.
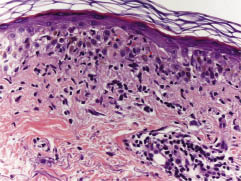
Laboratory tests showed slightly elevated C reactive protein (18 mg/l), erythrocyte sedimentation rate (22 mm/h), immunoglobulin E (174 IU/ml) and eosinophilia. A punch biopsy demonstrated a lymphohistiocytic infiltrate with occasional eosinophils in the superficial dermis and marked basal hydropic degeneration with cytoid bodies (colloid or Civatte bodies) identifiable within the basal epithelium and the papillary dermis (Fig. 2).
Fig. 2. Lymphohistiocytic infiltrate with occasional eosinophils in the superficial dermis and marked basal hydropic degeneration with cytoid bodies (colloid or Civatte bodies) (arrowed) identifiable within the basal epithelium and the papillary dermis. Haematoxylin and eosin (H&E) stain (original magnification ×400).
Alendronate was discontinued and treatment with oral steroids (1 mg/kg /bodyweight prednisone) was initiated. Six weeks later, the skin lesions had cleared without scarring. After 3 months of complete remission, symptoms recurred on re-challenge with alendronate at an identical dosage, and alendronate was therefore discontinued for second time. All skin lesions cleared fully after several weeks. Risedronic acid was initiated as an alternative treatment and no sensitization has been observed.
DISCUSSION
Alendronate is an effective anti-resorptive agent for the treatment of osteoporosis in postmenopausal women, as well as for treatment of vertebral fractures. Few cases of biphosphonate-associated cutaneous reactions have been reported in the literature (1). These skin reactions are usually scarce and are thought to be mediated by immunoglobulin E (1), and not histamine because, in most cases, side-effects developed several days after drug intake. In the case described here, skin lesions developed after 2 months of drug intake and showed a prolonged healing time after cessation of bisphosphonate treatment. It has been speculated that skeletal retention of the compound may play a role in this phenomenon (1). Phillips et al. (2) reported that alendronate challenge did not provoke a reaction in two patients with a previous urticarial reaction to pamidronate, while one patient was subsequently treated with clodronate without an untoward reaction. Equally, one patient sensitized to alendronate tolerated treatment with risedronate (3). These cases (2, 3) indicate that skin reactions to bisphosphonates are not a class effect; thus when a skin reaction is suspected to be due to sensitization to a specific bisphosphonate this should not inevitably preclude the use of these potent substances because different bisphosphonates with variant molecular structures may provide a safe alternative for the patient. Our patient, who had sensitization to alendronate, tolerated the chemically different risedronic acid well during long-term treatment. Reported skin reactions to alendronate also include lichen planus (4), superficial gyrate erythema (5), papulo-petechial skin eruption (6) and superficial perivascular spongiotic dermatitis (3). It is noteworthy that the clinical drug reaction in the present case was not suggestive of lichen planus, but subsequent histological study demonstrated that it was lichen planus.
The authors declare no conflict of interest.
REFERENCES