Lars Falk
R&D Department of Local Health Care, County of Östergötland, and Department of Dermatology and Venereology, Linköping University Hospital, Linköping
University, Linköping, Sweden



Lars Falk
R&D Department of Local Health Care, County of Östergötland, and Department of Dermatology and Venereology, Linköping University Hospital, Linköping
University, Linköping, Sweden
The overall agreement between different criteria for cervicitis in women infected with Chlamydia trachomatis and/or Mycoplasma genitalium, and in women who tested negative was examined. Women attending a clinic for sexually transmitted diseases were enrolled because of sexual partners’ suspected chlamydia infection. M. genitalium was tested in a sample of first-catch urine and an endocervical specimen, whereas specimens from four different sites were used for detection of C. trachomatis. Signs of friability and purulent endocervical discharge were documented at gynaecological examination. Specimens for microscopy were taken from the endocervix and urethra as well as the vaginal discharge, and bacterial vaginosis was examined for. The criteria being evaluated included cervical friability and/or pus; polymorphonuclear leukocytes (PMNL)/epithelium cell ratio in the vaginal discharge; and more than 30 PMNL per high-power field in the endocervical smear. The overall agreement of the indicators of cervicitis in women infected with C. trachomatis and/or M. genitalium was 40.5% (15/37), and for those women with negative tests 35.3% (12/34). The criteria for cervicitis require further evaluation, including study of a control group of women at low risk of having a sexually transmitted infection. Key words: mycoplasma genitalium; chlamydia; women; cervicitis; urethritis; bacterial vaginosis.
(Accepted May 7, 2010.)
Acta Derm Venereol 2010; 90: 506–511.
Lars Falk, R&D Department of Local Health Care, County of Östergötland, SE-581 85 Linköping, Sweden. E-mail: lars.falk@lio.se
Neisseria gonorrhoeae has largely obvious clinical signs of infection (1), with purulent discharge and diplococci detectable in stained slides by microscopic examination. Nowadays, Chlamydia trachomatis is the most common known cause of bacterial sexually transmitted infection (STI) worldwide, and the genital infection is mostly asymptomatic, especially in women (2, 3). Mycoplasma genitalium has, in the last decade, been shown to be an STI and an important and common cause of cervicitis, endometritis and, at least occasionally, also of salpingitis with possible tubal factor infertility (2, 4–9). Neither C. trachomatis nor M. genitalium can be visualized by light microscopy, but may cause urethritis. In men, urethritis can easily be visualized in a stained urethral smear (≥ 5 polymorphonuclear leucocytes (PMNL) in ≥ 5 high-power fields (HPF, magnification ×1000)) with a 90% sensitivity, but low specificity (10). The difficulty for the physician is to decide whether the inflammation is bacteral, and whether treatment with antibiotics and examination and treatment of the current partner is needed.
As Brunham et al. (11) stated in 1984, the lack of wide acceptance of objective criteria for cervical inflammation impedes clinical diagnosis. He and co-workers found that visualization of yellow mucopurulent endocervical discharge and the presence of ≥ 10 PMNL per HPF in endocervical smears correlated independently with C. trachomatis infection. In 1988 a similar correlation was found by visualization of friability of the endocervix in women infected with chlamydia, but it was also stated that other findings must be utilized (12). Weström & Mårdh (13) found that women with salpingitis and endometritis had more PMNL than epithelial cells in vaginal wet smears. Other definitions of endocervicitis have been proposed, and one commonly used and often recommended is the finding of more than 30 PMNL per HPF in the endocervical smear (14).
The aim of the current study was to evaluate overall agreement between different proposed definitions of cervicitis, such as friability/pus from the endocervix; more PMNL than vaginal epithelial cells in vaginal wet smear; and more than 30 PMNL per HPF in the endocervical smear. A secondary aim was to estimate microscopic findings of bacterial vaginosis, urethritis and risk-behaviour in women attending a clinic for sexually transmitted diseases (STD) because of their current or previous partner’s suspected chlamydia infection, and to compare these findings with those of a group of young women attending for Papanicolaou (Pap) smear screening.
METHODS
Patients
Women attending the STD clinic in Norrköping, Sweden, a city of 130,000 inhabitants, in October 2007 to January 2009, due to former or current partners’ verified or suspected chlamydia infection, were enrolled. They were a part of a multi-centre study evaluating the sensitivity of patients’ self-sampled vaginal specimen, first-catch urine (FCU), combined vaginal and FCU specimens, and endocervical specimens for detecting genital chlamydial infection in women (15). Data were collected on a detailed standard questionnaire regarding the reasons for attendance; age; symptoms (vaginal discharge, urethral pain during micturition, intermenstrual or post-coital bleeding, and lower abdominal pain); previous STIs; contraceptive method; numbers of sexual partners during the previous 12 months and antibiotic usage (type and indication of treatment) during the last month.
In a previous study in 2002, 157 women in the age range 22–26 years, in the national cervix screening programme for Pap smear were asked to participate in a study comparing the definitions of cervicitis (2). The reasons for not participating are described by Falk et al. (2). A total of 59 women (38%) participated, but two were excluded from comparison because of a chlamydia infection and missing data for an overall comparison, respectively. These 57 subjects served as controls with a “normal” STI risk.
Sampling and microbiological analysis
All patients were asked not to micturate within one, preferably 2 hours before sampling. Informed consent was given to a nurse, who also gave the patient information in writing and orally about the sampling procedure. The procedure of sampling for C. trachomatis has been described in detail previously, as have the nucleic acid amplification tests (NAATs) used (15). The four samples; i.e. vaginal, endocervical, FCU and a vaginal swab in FCU, were taken and sent by post to the Department of Laboratory Medicine, Microbiology Section, Örebro University Hospital, Örebro. The FCU sample was taken prior to the examination and placed in 13 ml polypropylene Sarstedt tubes. During the subsequent examination a physician used a swab for endocervical sampling. The physicians also sampled endocervical, urethral smears (taken with a blunt curette) and vaginal wet smear for microscopic examination. When sampling for M. genitalium, an endocervical specimen was taken with a polyacrylamide swab (Copan, Brescia, Italy), after the sampling for C. trachomatis, and the swab was placed in one of the FCU-containing tubes. This combined sample has been shown to be accurate in a previous study (16). The specimens were sent to Department of Clinical Microbiology, Linköping University Hospital. A 2 ml volume of the FCU was concentrated by centrifugation. The supernatant was discarded and 10 μl of proteinase K was added to the remaining 200 μl of urine and pellet, vortexed and incubated at 65ºC for 30 min. The mixture was extracted in a GenoM-48 (Genovision, Oslo, Norway) with the MagAttract DNA Mini M48 kit from Qiagen (Hilden, Germany). The samples were analysed in a Rotor-Gene 3000A (Corbett Research, Sydney, Australia) with 9 μl FCU extract in a 25 μl total reaction volume containing Smart Kit (Eurogentec, Seraing, Belgium), primers MgPa-355F and MgPa-432R and 6-carboxyfluorescein-labelled MgPa-380 minor groove binder probe. The instrument was programmed to a cycle of 50ºC for 5 min, 95ºC for 15 min and 45 cycles of denaturation at 95ºC for 15 s, and annealing and extension at 60ºC for 1 min. The primers amplified a 78-bp fragment in the MgPa operon.
All smears were examined with a ZeissTM (standard14) light microscope. Wet smears and methylene blue stained smears were examined in phase contrast 400 times and in 1000 times magnification, respectively. Amsel’s criteria were used for the diagnosis of bacterial vaginosis (17). All but three patients (n = 86) were examined by the author.
For the women in the “normal” STI risk group (n = 59, median age 24 years) all patients were examined by the author. The procedure for sampling for microscopy (Nikon Labophot) and M. genitalium and C. trachomatis analysis with PCR (FCU and endocervix) were similar to that in the present study (2). In 2002 the new variant strain of C. trachomatis (nvCT) had not been discovered. It may have existed, but the number of infected persons in Sweden at that time was presumably very small (18). It can thus be assumed that the NAAT used (Roche Cobas Amplicor C. trachomatis test) did not miss many, if any, chlamydia-infected woman because of the nvCT strain.
Statistical analyses
Fisher’s exact test and odds ratio were used to test differences in proportions and a t-test was used for testing differences in means (SPSS version 17.0, IBM, Chicago, IL, USA).
Results
Eighty-six women, age range 14–45 years (median age 22 years), were enrolled. A positive C. trachomatis test was found in 37 women (age range 14–38 years, median 21 years). Of those, 35 were tested for M. genitalium and 6 of these were shown to have a concurrent M. genitalium infection (17.1%) (Table I). Among the 49 C. trachomatis test negative women 6 had an M. genitalium infection (12.2%). In the group of 43 women with negative tests for M. genitalium and C. trachomatis 3 had received antibiotic treatment (amoxicillin, doxycycline and pivampicillin, respectively) during the last month and were thus excluded.
Symptoms of infection were reported in one-third of patients (26/83). There were no statistically significant differences in presence of symptoms between the groups positive for M. genitalium or C. trachomatis or not (Table I). Bacterial vaginosis was found in 43 of 83 women (51.8%) and in 22 of 37 (59.4%) chlamydia-infected women (Table I). Culture for Neisseria gonorrhoeae was negative for the 3 patients tested. None of the smears in the 83 women examined showed intracellular diplococci.
Urethritis (≥ 5 PMNL per HPF) was detected in 42% (15/36) of chlamydia-infected women compared with 15% (6/40) of women with negative tests for C. trachomatis and M. genitalium (p = 0.02) (Table I). If the cut-off for urethritis was determined as ≥ 10 PMNL per HPF the difference between the groups was more obvious: 28% (10/36) and 2.5% (1/40) respectively (p = 0.005) (Table II). Urethritis (≥ 5 PMNL/HPF) was seen in 10 women (17.5 %) in the “normal” STI risk group, i.e. the women in the national cancer screening group (n = 57), and in 4 (7%) with smear ≥ 10 PMNL/HPF. In comparison with chlamydia-infected women this showed a statistically significant difference (p = 0.02 and p = 0.01, respectively). No statistically significant differences in signs of urethritis were seen when those with negative tests (n = 40) were compared with the “normal” STI risk group of women (n = 57) (p = 0.60 and p = 0.96, respectively) (Table II).
Table I. Women enrolled at the sexually transmitted diseases (STD) clinic in Norrköping (n = 86). Symptoms (self-reported pain during micturition and/or discharge and/or intermenstrual bleeding and/or lower abdominal pain); and clinical and microscopic signs are shown. Antibiotic treatment had been given during the month prior to examination to three women with negative tests (n = 43), and hence they were excluded in comparisons of signs and symptoms
| Urethral smear (PL/HPF) | Cervical smear (PL/HPF) | Friability/pus | Wet smear | Symptoms Count (%) | Bacterial vaginosis Count (%) | |||||||||||||
| ≥ 5 (%) | < 5 (%) | UND (n) | ≥ 30 (%) | < 30 (%) | Yes (%) | No (%) | Unsurea (n) | PL>E (%) | PL≤E (%) | WND (n) | ||||||||
| C. trachomatis positive (n = 31)b | 45 | 55 | 0 | 52 | 48 | 50 | 50 | 3 | 53 | 47 | 1 | 10 (32) | 18 (58) | |||||
| M. genitalium positive (n = 6) | 17 | 83 | 0 | 0 | 100 | 40 | 60 | 1 | 17 | 83 | 0 | 2 (33) | 2 (33) | |||||
| Both above positive (n = 6) | 20 | 80 | 1 | 50 | 50 | 33 | 67 | 0 | 60 | 40 | 1 | 2 (33) | 4 (67) | |||||
| Negative tests (n = 40)c | 15 | 85 | 0 | 30 | 70 | 33 | 67 | 4 | 26 | 74 | 2 | 12 (30) | 19 (47) | |||||
| Total (n = 83)b | 27 | 73 | 1 | 37 | 63 | 40 | 60 | 8 | 38 | 62 | 4 | 26 (31) | 43 (52) | |||||
aDue to menstruation not possible to evaluate (n = 8).
bTwo women were not tested for M. genitalium.
cWomen tested due to partners’ chlamydial infection, but with negative results for C. trachomatis and M. genitalium.
PL: polymorphonuclear leucocytes; HPF: high-power field (1000×); E: (vaginal) epithelial cells; UND: microscopic examination of urethral smear not done; WND: microscopic examination of vaginal wet smear not done or signs not noted in case-notes. For the diagnosis of bacterial vaginosis Amsel’s criteria were used.
Table II. Signs of bacterial vaginosis, urethritis and cervicitis. Women enrolled at the sexually transmitted diseases clinic in Norrköping (n = 83). Clinical and microscopic signs. Women in a national cervical cancer screening group (n = 57) serving as a comparison group of cervicitis, urethritis and bacterial vaginosis. The table is dichotomized as to whether there was a bacterial vaginosis (BV). Alternative cervicitis definitions studied: having more polymorphonuclear leucocytes (PL) than vaginal epithelium cells in vaginal wet smear; friability/pus of portio cervicis; more than 30 PL per high-power field (HPF) (1000× magnification) in endocervical smear (i.e. by any definition). The table shows whether any or none of the definitions were fulfilled
| C. trachomatis (n = 31)a | Positive for: | Negative tests (n = 40) | Papanicolaou smear (n = 57) | Totalcd (n = 140) | |||||||||||||||||||||||||||||||
| Both (n = 6) | M. genitalium (n = 6) | ||||||||||||||||||||||||||||||||||
| Urethral smear | Cervicitis (PL/HPF) | Urethral smear | Cervicitis (PL/HPF) | Urethral smear | Cervicitis (PL/HPF) | Urethral smear | Cervicitis (PL/HPF) | Urethral smear | Cervicitis (PL/HPF) | Urethral smear | Cervicitis (PL/HPF) | ||||||||||||||||||||||||
| ≥ 10 | 5–9 | < 5 | Any | None | ≥ 10 | 5–9 | < 5 | Any | None | ≥ 10 | 5–9 | < 5 | Any | None | ≥ 10 | 5–9 | < 5 | Any | None | ≥ 10 | 5–9 | < 5 | Any | None | ≥ 10 | 5–9 | < 5 | Any | None | ||||||
| BV: Yes (n = 51)b | 8 | 2 | 8 | 12 | 5 | 0 | 1 | 2 | 3 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 4 | 14 | 15 | 3 | 1 | 1 | 6 | 4 | 4 | 10 | 9 | 31 | 35 | 14 | |||||
| BV: No (n = 89)c | 2 | 2 | 9 | 8 | 2 | 0 | 1 | 1 | 2 | 0 | 0 | 0 | 4 | 1 | 2 | 0 | 1 | 20 | 9 | 9 | 3 | 5 | 41 | 15 | 34 | 5 | 9 | 75 | 35 | 47 | |||||
| Total (n = 140)c,d | 10 | 4 | 17 | 20 | 7 | 0 | 2 | 3 | 5 | 1 | 0 | 1 | 5 | 2 | 3 | 1 | 5 | 34 | 24 | 12 | 4 | 6 | 47 | 19 | 38 | 15 | 18 | 106 | 70 | 61 | |||||
aTwo women were not tested for M. genitalium. A further two women without BV could not be compared because of concurrent menstruation making evaluation of portio cervicis difficult.
bOne woman (M. genitalium and C. trachomatis-positive) denied permission for a urethral smear; three chlamydia infected women (one both C. trachomatis and M. genitalium positive) could not be compared by all definitions of cervicitis due to menstruation or missing data in case-notes (however two had cervicitis by any definition). Three women with negative tests could not be compared by all definitions but two had signs of cervicitis by at least one definition.
cSix women could not be compared by all definitions of cervicitis, two with chlamydia infection, one with M. genitalium infection and three with negative tests. None of these had other signs of cervicitis.
For the diagnosis of BV Amsel’s criteria were used.
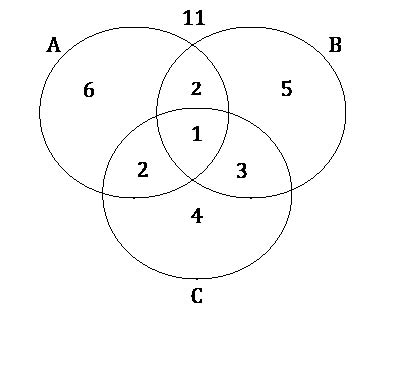
If our three instruments for defining cervicitis were ideal and there were no other causes of cervicitis than M. genitalium, C. trachomatis or N. gonorrhoeae, the “normal” STI risk group of 57 women would fall outside the circles in Fig. 1, provided that they had no other (non-infectious) risk of having a cervicitis. In fact, 37 women from the control group were outside the circles and the remaining 20 were scattered within the circles. Two were in all circles, giving an overall agreement of the proposed definitions of 68% (39/57) (Fig. 1). The overall agreement of three compared definitions of cervicitis in C. trachomatis and/or M. genitalium infected eligible women was 40.5% (15/37) (Fig. 2) and for those eligible women with negative tests 35.3% (12/34) (Fig. 3).
Fig. 1. A comparison group of 59 women (age range 22–26 years) attending the national cervical cancer screening programme for Papanicolaou smear and accepting enrolment in a study comparing cervicitis definitions. Two were excluded due to chlamydial infection and missing data for overall comparison, respectively. Circles represent fulfilment of criteria: A: friability of the portio and or endocervical pus; B: more than 30 polymorphonuclear leucocytes per high-power field in endocervical smear; C: more polymorphonuclear leucocytes than vaginal epithelial cells in vaginal wet smear. The number outside all circles represents those patients with no sign of endocervicitis by any studied definition.
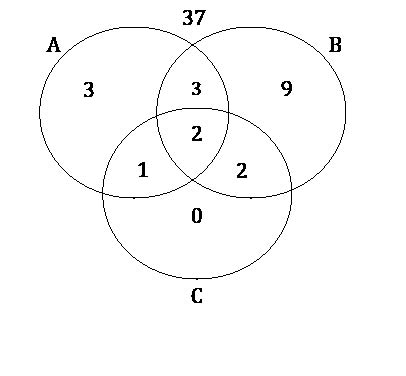
Fig. 2. C. trachomatis and/or M. genitalium infected women (n = 43) and the outcome and agreement using three different proposed definitions of cervicitis. In six women all three criteria could not be compared because of menstruation (n = 4) or lack of information in case-notes (n = 2). Thus, the findings from 37 women were compared. Circles are defined as in Fig. 1.
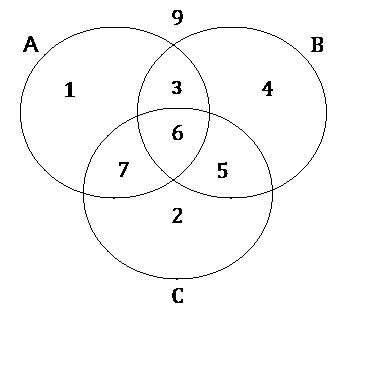
Fig. 3. Women (n = 34) with negative tests for C. trachomatis and/or M. genitalium attending because of their sexual partners’ suspected or verified chlamydia infection. The outcome and agreement using three different proposed definitions of cervicitis. Circles are defined as in Fig. 1. The number outside all circles represents those women with no sign of endocervicitis by any studied definition. Initially 43 women were eligible. In six women all three criteria could not be compared because of menstruation (n = 4) or lack of information in case-notes (n = 2). A further three women were excluded due to use of antibiotics during the last month. The number outside all circles represents those patients with no sign of endocervicitis by any studied definition.
Sensitivity, specificity, predictive positive value (PPV) and negative predictive value (NPV) in this population with high chlamydia prevalence (45.1%, 32/71) were for “vaginal wet smear” 54%, 70.6%, 66.7%, 58.5%, “endocervix stained smear more than 30 PMNL/HPF” 48.6%, 67.6%, 62.1%, 54.8% and “pus/friability of portio cervicis” 45.9%, 67.6%, 60.7%, 53.5%, respectively (Table III).
If those women with C. trachomatis and/or M. genitalium infection (n = 37) were compared with the “normal” STI risk group of 57 women, the specificity, PPV and NPV were higher and especially for “vaginal wet smear”, reaching 91.2% (52/57), 80% (20/25) and 75.4% (52/69), respectively (Table III, Figs 1 and 2).
Table III. Three different definitions of cervicitis, i.e. pus/friability of portio cervicis (A); endocervix smear with more than 30 polymorphonuclear leucocytes per high-power field (B); and vaginal wet smear with more polymorphonuclear leucocytes than vaginal epithelial cells (C). Sensitivity, specificity, predictive positive value (PPV) and negative predictive value (NPV) of these definitions were compared in women with C. trachomatis and/or M. genitalium infection (n = 37) and women enrolled in the study at high risk of infection, but with negative tests for the bacteria (n = 34) (High risk group). These infected women (n = 37) were also compared with a “normal sexually transmitted infections (STI) risk group” of 57 women not infected with C. trachomatis or M. genitalium
| Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | ||
| High risk group (n = 71) | A | 45.9 | 67.6 | 60.7 | 53.5 |
| B | 48.6 | 67.6 | 62.1 | 54.8 | |
| C | 54.0 | 70.6 | 66.7 | 58.5 | |
| ”Normal STI risk group” (n = 94) | A | 45.9 | 84.2 | 65.4 | 70.6 |
| B | 48.6 | 71.9 | 52.9 | 68.3 | |
| C | 54.0 | 91.2 | 80.0 | 75.4 | |
Data for use of hormonal contraceptives, number of recent sexual partners and history of STIs for the 71 eligible women, age range 14–45 years (median age 21 years), shown in Figs 2 and 3 are presented in Table IV. Two-thirds of all women used a safe contraceptive method (66.2%) and no differences could be seen between the sub-groups (Table IV). There were no significant differences in risk-taking measured by number of partners during the last year, smoking habits, previous induced abortions or previous STIs between those infected with M. genitalium or C. trachomatis and those not infected (Table IV). The M. genitalium infected women (n = 10) were older (p = 0.09), but with a wide range. In the “normal” STI risk group of 57 women the use of hormonal contraceptives was 64.9%, which is similar to the other groups compared in this study. Other mentioned risk factors were not asked for.
Table IV. Women enrolled at the sexually transmitted diseases (STD) clinic in Norrköping due to sexual partners’ suspected chlamydia infection and of whom proposed criteria for cervicitis were compared (n = 71). Use of contraceptives, smoking habits, number of sexual partners previous 12 months, history of previously diagnosed sexually transmitted infections (STIs), previous induced abortions and age
| Contraceptive method | Smokinga | Sexual partnersb | Previous STIs | Induced abortions | Age (years) | ||||||||||||||||||
| C. trachomatis | Other | ||||||||||||||||||||||
| CP | G | IUD | Noc | Yes | No | Md | Mean | Range | Yes | No | Yes | No | Yes | No | Md | Mean | Range | ||||||
| C. trachomatis pos (n = 27)d | 9 | 8 | 1 | 9 | 13 | 14 | 3 | 3 | 1–8 | 12 | 15 | 3 | 24 | 6 | 21 | 21 | 21 | 14–33 | |||||
| M. genitalium pos (n = 5) | 1 | 1 | 0 | 3 | 2 | 3 | 3 | 3.5 | 1–6 | 2 | 3 | 0 | 5 | 2 | 3 | 23 | 26.5 | 22–33 | |||||
| Both above positive (n = 5) | 0 | 3 | 0 | 2 | 2 | 2 | 2 | 3 | 2–6 | 1 | 4 | 2 | 3 | 2 | 3 | 22 | 24 | 16–38 | |||||
| Negative tests (n = 34) | 11 | 9 | 4 | 10 | 14 | 19 | 2 | 2.5 | 1–10 | 12 | 22 | 4 | 30 | 11 | 23 | 21.5 | 24.5 | 16–45 | |||||
| Total (n = 71)d | 21 | 21 | 5 | 24 | 31 | 38 | 2 | 3 | 1–10 | 27 | 44 | 9 | 62 | 21 | 50 | 21 | 23.5 | 14–45 | |||||
aData lacking from two women (M. genitalium and C. trachomatis positive and negative in all tests, respectively).
bData lacking from one woman (negative in all tests).
cNo method or condom occasionally.
dTwo women were not tested for M. genitalium.
Md: median; CP: combined oestrogen and gestagen method, G: gestagen method; IUD: intrauterine device.
All women in the study (n = 140) were compared regarding urethritis and cervicitis in a dichotomy as to whether there was a bacterial vaginosis, and compared within the subgroups: those with negative tests (n = 40); those with M. genitalium and/or C. trachomatis infection (n = 43), or those belonging to “normal” STI risk group of women (n = 57) (Table II). No statistically significant differences could be seen between those women with and without bacterial vaginosis in the different subgroups. In the group as a whole (49 women with bacterial vaginosis and 82 not having bacterial vaginosis); however, there were more women with bacterial vaginosis who had at least one of proposed definition of a cervicitis fulfilled (OR 3.36 (95% confidence interval (CI) 1.57–7.17)). Urethritis (≥ 5 PMNL/HPF) was also more common among women having a bacterial vaginosis (n = 50) than among those not (n = 89) (OR 3.28; 95% CI 1.46–7.36) (Table II).
Discussion
Bacterial vaginosis was found in more than half of the women with chlamydia, and this finding is in good agreement with other studies (2, 19–21). There was, however, no significant difference between those with M. genitalium or C. trachomatis infection, and those not infected. The reason could be that those not infected were not a low-risk group for an STI. In the “normal” STI risk group of women, however, bacterial vaginosis was, as expected, considerably lower. This group can be assumed to be an average group of women in terms of risk-taking for contracting an STI.
The definitions of cervicitis in a clinical setting are not ideal. The evaluated definitions, as proposed in the literature, showed comparable outcome in this study. Although some of the definitions have been studied (14), they have not previously been compared simultaneously. The sensitivity of finding a cervicitis by any definition for detecting chlamydia infection reached only 76% (25/33). Even more distressing was the low predictive positive value and the low specificity for the different compared definitions of cervicitis. The latter findings could be explained as a selection bias. All women enrolled in the present study were selected because of their presumably high risk of having a chlamydia infection. The comparison group (those negative in tests (n = 34) was not necessarily at low risk for STI and thus cervicitis. This is supported by the fact that there were no differences measured in risk behaviour, such as number of sexual partners, previous STIs, or history of induced abortions between the groups. When comparing the study’s M. genitalium and/or C. trachomatis infected women with the “normal” STI risk group from the general population, the specificity, PPV and NPV for cervicitis, by any definition, was still low (between 53% and 91%). In fact, the vaginal wet smear seemed to be the most accurate method of predicting infection.
Urethritis, defined as ≥ 5 PMNL per HPF, was significantly more frequent among the women with chlamydia infection. This has previously been reported in a Norwegian study of an STI-clinic population, in which 72% of those infected with chlamydia had a urethritis, compared with 49% (OR 3.6, 95% CI 3.0–4.4) of those not having a M. genitalium or C. trachomatis infection (19). Similar differences were seen also in a Swedish study (2).
Bacterial vaginosis has been discussed over the years as to whether it is a functional disorder or a result of specific pathogen bacteria (22). The statistically significant higher levels of urethritis and cervicitis in women with bacterial vaginosis in this study might be caused by the high number of M. genitalium or C. trachomatis infection in the high-risk-taking group of women (n = 83) compared with the low prevalence of bacterial vaginosis and signs of cervicitis and urethritis in the studying probably more average STI risk-taking group of women (n = 57). The number of patients, however, in the five subgroups when OR was calculated was too small to demonstrate a statistically significant difference (the power was too low). If, on the other hand, M. genitalium or C. trachomatis infections were not confounders, then the significant OR for having a urethritis or cervicitis in women with bacterial vaginosis could be interpreted as a true relationship. These findings need to be studied further.
The interpretation of smears depends on several variables independently of whether stained dry smears or wet smears are examined: the instrument for sampling, the standard of the microscope, how the microscope is used and the experience of the clinician. Whichever strict protocol is used, a degree of subjectivity in interpretation will remain. More studies are required on the diagnostic tools for determining the clinically relevant definition of cervicitis. Women at low risk of having an STI and with few lifetime partners would be a suitable group for comparison.
In summary, the criteria defining cervicitis are currently inadequate and further studies to evaluate the diagnostic criteria used worldwide are urgently needed. More studies on the role of bacterial vaginosis in cervicitis and urethritis are also warranted.
Acknowledgements
I am most grateful to the staff at the STD clinic in Norrköping (especially to Margreth Wastesson, Jeanette Groenheit and Ylva Zander). I also thank Erik Kihlström for information about the laboratory testing procedure of specimens tested for M. genitalium and for valuable comments on the first draft of the manuscript. I thank Chris Anderson for linguistic revision of the manuscript and for scientific comments. I am also most grateful to Lars Valter for statistical computations.
The study was approved by the regional research ethics committee of Linköping on 9 August 2006 (M 112–06) and was funded by the Medical Research Council of Southeast Sweden, ALF grants from the County Council of Östergötland and by the Department of Communicable Disease Control, County of Östergötland.
The author declares no conflict of interest.
References

