Melek Kesir Koç1, Sibel Südoğan1, Mukaddes Kavala1, Emek Kocatürk1*, Nesimi Büyükbabani2 and Sümeyye Altıntaş2
1Department of Dermatology, Göztepe Training and Research Hospital, and 2Department of Pathology, Istanbul University Istanbul Medical Faculty, Istanbul, Turkey. *E-mail: dremekozgur@gmail.com
Accepted April 28, 2010.
Spitz naevus is a melanocytic lesion that is characterized by neoplastic proliferation of epithelioid and/or fusiform-shaped cells. Rare variations of Spitz naevus, such as desmoplastic, hyalinizing, plexiform, pagetoid, pigmented fusiform and angiomatoid Spitz naevus have been described (1). Desmoplastic Spitz naevus (DSN), first described by Reed et al. in 1975 (2). Histopathologically, desmoplastic Spitz naevus is characterized by epithelioid and/or fusiform-shaped cells surrounded by a fibrous stroma consisting of thick bundles of collagen. It has clinical and histopathological features that are difficult to differentiate from dermatofibroma and desmoplastic malignant melanoma (DMM), which requires aggressive therapy for cure.
CASE REPORT
A 36-year-old female patient was admitted with a swelling on her right leg, which was not accompanied by any subjective complaints or previous history of trauma, that had been growing slowly for 4 months. On examination a raised, well-circumscribed, red-brown nodular lesion of approximately 1 cm diameter was observed anteromedially on the right knee. A total excision was performed.
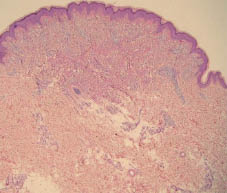
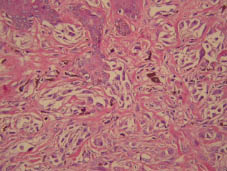
Histopathological examination (Figs 1 and 2) revealed a slight acanthosis in the epidermis, a symmetrical lesion consisting of melanocytes, in fusiform and epithelioid morphology and spitzoid in appearance, surrounded by hypereosinophilic bundles of collagen starting from the papillary dermis and reaching the mid-reticular dermis, and a slight lymphocytic infiltration around the vessels. Immunophenotypical examination revealed a stronger positive staining in the superficial, and a weaker positive staining in the deep portions of the lesion for S-100, Melan A, and HMB-45. Ki-67-positive reaction was observed mostly on perivascular lymphoid cells in the dermis, while it was observed in melanocytic cells at a level of 1–2%. Based on these findings, it was concluded that the lesion was a Spitz naevus, predominantly located in the dermis and associated with minimum junctional components, and which led to stromal desmoplasia. Subsequently, the patient was diagnosed with DSN. No recurrence was observed during the 2-year follow-up period after the total excision of the lesion with a 0.5 cm margin.
Fig. 1. Near-dermal lesion with laterally sharp border.
Fig. 2. Melanocytes with spitzoid appearance, stromal hypereosinophilic bundles of collagen and melanophages in the junctional region and superficial dermis (haematoxylin and eosin ×200).
DISCUSSION
DSN is an intradermal lesion, characterized by marked collagen production in the dermis. It is usually a red-brown papule or nodule, located on the extremities (3). However, lesions located on the abdomen, head and neck region and a case with multiple lesions have been reported (4). It is differentiated from classical variants of Spitz naevi by lack of dermoepidermal activity, absence of Kamino bodies, increased dermal collagen and presence of ganglion-like epithelioid cells (5).
The increased stromal fibrosis in the DSN has been considered as evidence of trauma or involution, and it has been suggested that the fibrosis is more pronounced in elderly patients (5, 6). However, in a series of 15 cases two 8-year-old children were detected to have similar stromal changes as seven adult patients over 30 years of age, and thus it has been concluded that the stromal changes are not age-related (5). In the present case, a 36-year-old woman, with no previous history of trauma, had had a lesion for 4 months.
The DSN can be mistaken for dermatofibroma due to similar location and clinical appearance. It can be differentiated precisely from dermatofibroma with the presence of melanocytes and the positive immunohistochemical staining of the cells with S-100 protein and antibody HMB-45 (5). Those histopathological findings were also positive for our patient.
DMM have been encountered recently due to the increasing incidence of melanoma. Unlike DSN located on the extremities of young adults, DMM is located on the sun-exposed skin of the head and neck of elderly patients (7). The age of our patient and the location of lesion were consistent with DSN. The accurate diagnosis of DSN requires an experienced pathologist and immunohistochemical examination. Histologically, DMM consists of abundant collagen fibres and fusiform-shaped melanocytes with pleomorphic nuclei. Unlike DSN, DMM elicits cellular atypia and marked inflammatory response. On immunophenotypic examination, positive HMB-45 and Melan-A staining in Spitz naevus and negative HMB-45 and Melan-A staining in DMM is useful in the differential diagnosis (7, 8). In addition, the number of Ki-67 positive cells that indicates proliferative activity is much higher in DMM than in Spitz naevus (3). The young age of our patient, extremity located lesion, positive HMB-45 and Melan-A staining, cellular atypia in melanoma, mitosis, marked lymphocyte infiltration and the absence of positive Ki-67 staining are findings that facilitate the differential diagnosis of Spitz naevus from DMM.
REFERENCES