Patients with autoimmune urticaria (AIU) and positive autologous serum skin test (ASST) represent a more serious type of chronic urticaria that does not respond to treatment with antihistamines, but responds completely to systemic corticosteroids. Because of the chronic course of the disease, there is a risk of side-effects. Cyclosporin A (CsA) is an alternative treatment for patients with AIU. In order to determine the efficacy of CsA at the lowest possible dose in patients with chronic idiopathic urticaria and positive ASST, 30 patients were included in a 5-month study with a follow-up one year after the end of treatment. All patients had positive ASST before treatment and autoantibodies were present in 73%. Twenty-three patients completed the study and responded to low-dose CsA treatment. Three patients did not respond to a dose of 2.5 mg/kg CsA, and 4 patients dropped-out due to side-effects. After the first month of treatment, an improvement of 31% was noted, reaching 88% after the fifth month of treatment. The mean dose of CsA was 2.16 mg/kg for the first month and 0.55 mg/kg for the fifth month. Three to 6 months after the end of the study, the ASST was repeated and was negative in 78.3% of patients. At the one-year follow-up, 20 patients were symptom-free (87%) and 3 had relapsed (13%). CsA, even in low-doses, can be an effective and short-term treatment with minimum side-effects in patients with AIU. Key words: urticaria; autoimmune diseases; cyclosporin; skin tests.
(Accepted May 11, 2010.)
Acta Derm Venereol 2011; 91: 50–54
Alexandra Katsarou, 1st Department of Dermatology and Venereology, National and Kapodestrian University of Athens, 5 I. Dragoumi St., GR-16121 Athens, Greece. E-mail: cboubouka@gmail.com
Chronic urticaria is defined as the daily or almost daily occurrence of wheals for at least 6 weeks. It remains a challenge in terms of aetiology, investigation and management. The term includes physical urticarias, chronic idiopathic urticaria and urticarial vasculitis (1). Chronic urticaria can be due to physical factors (10–20%), drugs (or drug additives) (2), foods (3) food preservatives, infections (bacteria, viruses, fungi) (4), parasites, inhalants (dust, animal fur, pollen), internal diseases (systemic lupus erythematosus (SLE), rheumatoid arthritis, thyroiditis, polymyositis) (4, 5) and psychological stress. A specific aetiological factor can be found in approximately 20–30% of patients with chronic urticaria, whereas in the remaining 70–80% the cause is not identifiable. The term chronic idiopathic urticaria (CIU) is used in situations in which an aetiological factor has not been identified and urticarial vasculitis and predominant physical urticarias have been excluded. Thirty to 50% of CIU is of autoimmune origin. Autoimmune urticaria (AIU) seems to have a high prevalence in children too, being responsible for approximately 30% of cases of CIU in this group (6).
It has been established that 30–50% of patients with CIU have circulating autoantibodies directed against immunoglobulin E (IgE) or the alpha chain of the high-affinity IgE receptor (Fc epsilon RI), (7, 8), which may play a role in the activation of the final common pathway in urticaria: mast cell activation and degranulation (9). The antibodies can be detected indirectly, either in vivo by cutaneous tests with serum injections (autologous serum skin test (ASST)) or in vitro by serum-induced basophil histamine release (HR-urticaria test) (6, 10). Patients with AIU represent a more serious type of chronic urticaria that does not respond to treatment with antihistamine doses above the usual daily recommendations, but responds completely to treatment with systemic corticosteroids. Because of the chronic course of the disease, there is a risk of side-effects from this type of treatment. Cyclosporin A (CsA) is an alternative treatment to corticosteroids because it inhibits cell-mediated immunity by down-regulating Th1 lymphocyte responses and antibody formation and inhibits the release of mast-cell mediators (11, 12).
The aim of this study was to determine the efficacy of CsA in a treatment using the lowest possible dose in patients with autoimmune urticaria and ASST. Follow-up was performed one year after the end of treatment to establish the lasting effect of treatment as well as the response of the ASST.
MATERIALS AND METHODS
Patients with CIU attending the Dermatology Department of “Αndreas Sygros” University Hospital, Athens, Greece were invited to participate in this prospective, controlled, open-label study. The study was approved by the ethics committee and there were no conflicts of interest.
Thirty patients with AIU were included in the study. The inclusion and exclusion criteria are listed in Table I.
Table I. Inclusion and exclusion critera of the study
|
Inclusion criteria
|
- Age 15 years and over, both genders and signing informed consent
|
- Individual history of active chronic idiopathic urticaria (CIU) for a period of 6 weeks or greater prior to study enrolment
|
- Resistance to antihistamines and response only to systemic corticosteroids
|
- Low or negative titres of basophils
|
- Positive autologous serum skin test
|
- Blood pressure and renal function within normal range
|
- Withdrawal of anti-inflammatory/anti-histamine therapy for a period of two weeks and one week, respectively, prior to study enrolment
|
- Patients compliant towards protocol specifications
|
- Negative Pap smear, normal abdominal ultrasound, normal mammography
|
|
Exclusion criteria
|
- Female patients being pregnant or lactating
|
- Patients receiving medications possible to intervene on study outcomes (sedatives, corticosteroids, immune system modulators, etc.)
|
- Substance abuse (e.g. alcohol)
|
- Patients with pruritus of known aetiology
|
- Patients whose laboratory tests exceed normal levels
|
- Patients with severe systemic diseases (cardiovascular, respiratory, renal, hepatic, nervous, etc., or any electrocardiographic abnormality identified)
|
- Patients with a history of malignancy
|
- Patients taking part in other clinical trial at any time during this study
|
- Hypertension (diastolic blood pressure greater than 95 mmHg)
|
During the initial visit (recruitment phase) patients provided written informed consent and were subjected to clinical and laboratory examination. Detailed medical history recording and specific clinical examination were carried out by the investigators to confirm the diagnosis and to exclude any urticaria of known aetiology, any physical or other type of inductive factor or any form of typical underlying pathology (e.g. Pap smear, abdominal ultrasound, mammography). Patients were screened for anti-nuclear antibody (ANA), anti-dsDNS, anti-TG, anti-TPO, against smooth muscle, anti-mitochondrial and against cells of the stomach wall. The patients underwent an ASST, performed by intradermal injection of 50 μl autologous serum, histamine (10 μg/ml) and 0.9% sterile saline, separately into the volar forearm. The distance between the injection sites was 3–5 cm, and the wheal and flare responses were measured at 30 min, as described previously (13). A wheal size of 9 mm or more in total (comparing it to the adjacent saline control skin test which makes a much smaller wheal). All patients had stopped any medication at least 3 days before the ASST was performed.
The patients enrolled in the study were instructed to check their blood pressure twice a week, and after two weeks they were subjected to laboratory examination (levels of blood urea nitrogen (BUN) and creatinine) and another visit was scheduled (V0) to establish the lowest possible initial dose of CsA. Clinical evaluation and follow-up were performed at baseline (V0), 1, 2, 3, 4 and 5 months (V1–V5).
At every visit, blood pressure, BUN and creatinine levels were measured. Renal function and blood tests were repeated every 15 days, and blood pressure was measured twice a week. The initial dose of CsA was between 1.5–2.5 mg/kg and was adjusted according to the clinical course of the patient and appearance of side-effects. The dose was decreased if creatinine increased more than 30% over baseline. If the results were persistent over two evaluations, CsA was discontinued. Blood pressure was considered elevated when diastolic blood pressure was greater than 105 mmHg on one occasion, or greater than 95mmHg on several occasions. The dose was then decreased, or anti-hypertensives were added (14). After the symptoms subsided (usually in the second month) and after a period of time without any or with slight symptoms (approximately one month) the CsA dose was reduced until the end of the study period (5 months). Clearance of symptoms or 5 months of treatment with CsA was considered as the end of the study. The ASST was repeated 3–6 months after the end of the study and a final follow-up was performed one year after the end of treatment.
Clinical assessment
Clinical evaluation, based on a scale of 0–3, was assessed as follows:
- Pruritus severity: the presence and severity of pruritus was assessed on a 4-grade scale (0 = absent, 1 = present, but not annoying, 2 = present, annoying but does not disturb everyday activities and/or sleep, 3 = present, annoying, disturbing everyday activities and/or sleep).
- Number of wheals in a 4-grade scale (0: no wheals, 1: 1–6 wheals, 2: 7–12 wheals, 3: > 12 wheals).
- The diameter of the largest wheal on a 4-grade scale (0 = no wheal, 1 = wheals with a diameter of up to 1.5 cm, 2 = wheals with a diameter between 1.5 and 3 cm, 3 = wheals above 3 cm in diameter).
- Average pruritus duration in a 4-grade scale (0 = no pruritus, 1 = pruritus lasting up to 6 h, 2 = pruritus duration between 6 and 12 h, 3 = pruritus duration above 12 h).
- Patients dropped out of the study due to intolerable side-effects, such as markedly elevated blood pressure or creatinine levels.
Statistical analysis
Between visits, the score of the individual signs and symptoms, as well as the total score were compared using a non-parametric test (Wilcoxon). The percentage improvement at each visit was calculated referring to the base score (V0). To describe the improvement, the median of each symptom was calculated at each visit. The prevalence of auto-antibodies at admission was also calculated.
RESULTS
The study included 5 men and 25 women. The age range of the patients was 18–70 years (mean ± SD, 47.6 ± 12.2 years) and the duration of urticaria ranged from 3 months to 25 years.
All patients had positive ASST before the treatment. Presence of autoantibodies was noted in 22 patients (73.3%). Of the initial 30 patients, 14 were positive against smooth muscle antibodies (46.7%). Antibodies against cells of the stomach wall were noted in 4 (13.3%) patients. Anti-TG and anti-TPO antibodies were noted in 10 (33.3%) patients, 10 had positive ANA (33.3%) and 3 positive anti-dsDNA (10%).
Of the 30 patients, 23 completed the 5-month study (76.7%) and responded satisfactorily to the low-dose CsA treatment. In 3 patients (11.5%) there was no response to a dose of up to 2.5 mg/kg and the patients stopped treatment after the third month. Of the 4 patients (13.3%) who dropped out due to high blood pressure, 3 were male.
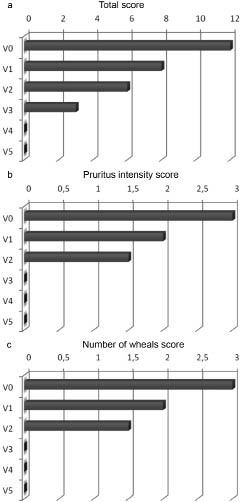
After the first month of treatment an improvement of 31% was noted, 46% after the second month, 71% after the third month, 87% after the fourth month and 88% after the end of the study. All of the partial symptoms that were considered in the patient’s evaluation (pruritus, number of wheals, size of wheals and duration of pruritus) improved substantially after the administration of CsA (Fig. 1a). A gradient drop was noted in the total score from visit to visit. Initially, it began with a median score of 12 (i.e., a majority of patients had maximal score for all four variables), which decreased until the end of the study, when the total score was 0. The score improvement was significant between V0 and V1 (p < 0.001), V1 and V2 (p < 0.001), V2 and V3 (p = 0.001), and V3 and V4 (p = 0.001), but was not significant between V4 and V5 (p = 0.16).
Fig. 1. Clinical results (median values) during the 5 months of cyclosporin treatment. (a) Total score of clinical signs and symptoms (including pruritus, no. of wheals, diameter of wheals and pruritus duration). (b) Pruritus intensity score. (c) Score for number of wheals. n = 30 for baseline and up to visit two (V0–V2) and n = 23 for the following visits (V3–V5). For evaluation of significance, see text.
Figs 1b–c show the improvement in the intensity of pruritus and number of wheals during the study. Pruritus severity improved 33% after the first month of treatment and 90% after the fifth month. An equivalent improvement was noted for the number of wheals, with a 33% improvement after the first month, and an 89% improvement at the end of the study. For both symptoms the median value of the score at admission (V0) was 3, after the first month (V1) 2 and after the second month (V2) 1.5. The median value of the score for both symptoms for visits V3–V5 was 0. This could be justified by the fact that the number of patients (n) after visit V3 was reduced to 23, due both to resistance to treatment and to side-effects.
Three to 6 months after the end of the study, the ASST was repeated in the 23 patients who completed the study. In 18 of these patients the ASST test was negative and clinical symptoms were absent (78.3%). Two patients had a positive ASST, but were symptom-free (8.7%), and 3 patients, despite having a negative ASST, had relapsed, presenting clinical symptoms (13%).
During the study the patients were given the lowest possible dose of CsA. The initial dose varied between 1.5 and 2.5 mg/kg and the dose was reduced every month according to the improvement in symptoms. In patients who did not respond to an initial dose of 2 mg/kg, the dose was increased to 2.5 mg/kg in the second month. In all patients the mean dose of CsA was 2.16 mg/kg for the first month, 1.92 mg/kg for the second month, 1.33 mg/kg for the third month, 0.83 mg/kg for the fourth month and 0.55 mg/kg for the fifth month.
Four patients dropped out due to high blood pressure (13.3%) at between 2 and 4 months, and the mean dose the patients were receiving at that time was 1.5 mg/kg. Of these 4 patients, 3 were responding to treatment and one was not. Additional side-effects were noted in 8 patients, but they remained in the study (arthralgias (n = 2), loss of appetite (n = 3), headache (n = 3)). All of the additional side-effects resolved, however, after reducing the dosage.
A second follow-up was conducted one year after the end of the treatment period. Of the 23 patients who had initially responded to treatment, 20 (87%) were free of symptoms and 3 (13%) had relapsed.
DISCUSSION
Treatment with CsA was well tolerated in the 23 patients who completed the study. This is of importance because CIU compromises the quality of life of patients. The major side-effect was elevated blood pressure, which caused 4 patients to drop out (even on a low dosage). Renal function was not affected in any of the patients. A significant improvement of 31% was noted after one month of therapy with a mean dose of 2.16 mg/kg, whereas an improvement of 88% was noted at the end of the study. The dose varied between 1.5 and 2.5 mg/kg, which is significantly lower than that used in psoriasis and other known dermopathies.
The treatment results were obtained over a period of 5 months, which is a relatively short time, and were sustained for at least one year.
Chronic AIU is caused by IgG antibodies to the α subunit of the IgE receptor, which probably plays a role in mast cell activation and release of both pre-formed and newly formed mediators. Mast cell degranulation also releases various chemokines and cytokines that are involved in urticaria formation. Skin biopsies reveal a perivascular infiltrate that surrounds small vessels within the superficial and deep dermis, with a prominence of CD4+ T-lymphocytes and monocytes (15). Neutrophils and eosinophils are both present. Clinical improvement in AIU after removal of autoantibodies by plasmapheresis and immunomodulatory therapy, as well as demonstration of association with human leucocyte antigen (HLA DR4), suggest that autoimmune mechanisms are involved in the pathogenesis of CIU (16).
The main mechanism of action of CsA consists in inhibition of HT-cell function. In stimulated T cells, CsA inhibits activation by suppressing IL-2 production and expression. This inhibition blocks the activation of T-helper cells, T-regulatory cells, natural killers and monocytes (17). The inhibition seems to be dose-dependent and also affects other calcium-dependent events, such as nitric oxide activation, cell degranulation and apoptosis (17). In stimulated mast cells, CsA decreases histamine release and there is decreased production of chemotactic factors and down-regulation of various cell adhesion molecules (18).
Because of its mechanism of action, CsA seems to be a very effective treatment in CIU, with only minor and dose-related side-effects.
The negativity of the ASST test 3–6 months after the end of treatment in 78.3% of patients is noteworthy, as it shows that treatment with CsA can cause suppression of the autoimmunity in a significant percentage of cases, lasting even after the end of the study. The fact that there were cases in which the ASST was negative but the patients had clinical symptoms indicates that ASST cannot be considered 100% reliable. However, it can be very helpful in situations in which the serum-induced basophil histamine release (HR-urticaria test) is not available.
Approximately 75% of patients with autoimmune urticaria in this study also had other autoantibodies. Autoantibodies are produced by B cells during physiological immune responses in elderly people and neonates. It is thought that they play a role in the elimination of denatured cells (19, 20).
In the present study patients were screened for anti-thyroid antibodies (anti-TG and anti-TPO), antibodies against smooth muscle, ANA, anti-dsDNA, anti-mitochondrial and against cells of the stomach wall. Twenty-two patients were positive for autoantibodies, the majority of whom were positive for antibodies against smooth muscle, ANA, anti-TPO and anti-TG. The correlation of chronic urticaria with thyroid disease, mainly Hashimoto’s thyroiditis, has been long-established (21, 22), but with H. pylori the results are controversial, although there is evidence of a correlation between H. pylori and chronic urticaria (23). Other autoantibodies that have been found in patients with chronic urticaria include mainly rheumatoid factor (24).
Previous studies of CsA in CIU (25, 26) have been for periods of 4 and 16 weeks, with doses between 3 and 5 mg/kg. In our study the treatment was longer (5 months) and the dose of CsA lower (1.5–2.5 mg/kg), which makes it much more tolerable, with minimum side-effects. A randomized, controlled study of CsA in CIU is warranted.
The authors declare no conflict of interest.
REFERENCES