Minh S. Luong1, Laurent Jomir2, Pierre Labauge2, Michel Dandurand1, Laurent Meunier1 and Pierre-Emmanuel Stoebner1*
Departments of 1Dermatology and 2Neurology, Groupe Hospitalo-Universitaire Caremeau, Place du Pr R Debre, FR-30029 Nîmes cedex 9, France. *E-mail: pierre.stoebner@chu-nimes.fr
Accepted May 18, 2010.
Ross syndrome is a rare partial dysautonomic syndrome of unknown aetiology, characterized by a one-sided or bilateral anhidrosis associated with Holmes-Adie syndrome (defined by tonic pupil and hyporeflexia of deep tendons) (1). Since it was first described in 1958 (2), approximately 50 cases have been described in the literature (3). Dermatologists may be confronted with this disorder of thermoregulation, which is often revealed by a segmental “compensatory” hyperhidrosis. We describe here a case of Ross syndrome associated with Sjögren syndrome (SS) and discuss the potential relationship between these two entities. Thermography imaging exploration with an infrared camera performed in different ambient temperature settings allowed better definition of the thermoregulatory sweating abnormalities in our patient. Moreover, to our knowledge, this examination showed, for the first time, an unexpected body “thermal pattern”, which may be characteristic of Ross syndrome.
Case report
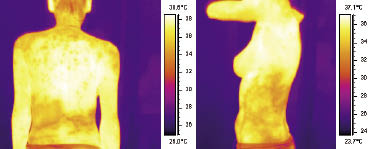
We present here a case of a 35-year-old woman with a 10-year medical history of localized hyperhidrosis. Her medical history revealed autoimmune thyroid disease and SS. The hyperhidrosis appeared at an ambient temperature of approximately 25–27°C and was localized on the left side of her lower back, extending belt-like towards the side and in the controlateral lower back on the right side, as well as on the nape of her neck and shoulders. The rest of the skin was anhidrotic. She was also heat intolerant, with lack of sweating, abnormal increase in body temperature and generalized fatigability when exposed to high ambient temperatures (32–34°C). Both pupils showed a slow reaction to light and a normal constriction to a near target, and deep tendon jerks were absent without motor deficits (Holmes-Adie syndrome). There were no other signs of autonomic dysfunction. Punch biopsies obtained from hyperhidrotic and hypohidrotic skin areas were normal. The skin direct immunofluorescence test was negative. Blood explorations showed an isolated presence of anti-SSA, anti-SSB antibodies and anti-thyroid antibodies. Serum ganglionic (AChR) antibody was negative. Oral and conjunctival Sicca were objectively confirmed by Schirmer’s test. Salivary gland biopsy revealed lymphocytic infiltration in both periglandular and perivascular regions. All of these Sicca findings fulfilled the diagnostic criteria for primary SS (4). Brain and spinal cord magnetic resonance imaging (MRI), as well as thoracic and abdominal computed tomography scan findings, were normal. Electrophysiological explorations of both hands and forearms showed an absence or collapse of the sympathetic skin responses. Nerve conduction study findings, EEG and cardiac tilt-test (reflecting the adrenergic sympathetic and parasympathetic functions) were normal. Thermographic explorations with an infrared camera (A320, FLIRsystems, Inc., Issy Les Moulineaux, France) allowed for evaluating the body’s surface temperature at 22°C and after a 20 min exposure to 32°C ambient temperature (Fig. 1). This examination was significantly more efficient than the Minor Starch Test and clearly delimited the skin thermoregulation abnormalities associated with Ross syndrome. Hyperhidrotic and anhidrotic areas were also clearly visualized as the lowest and highest estimated skin surface temperature. This examination showed large dermatomal-like patterns in hyperhidrotic areas (lower back and shoulder regions), but also detected unexpected smaller patch-like “lower temperature areas” on the upper back. The patient was informed about the limited success of treatments such as topical glycopyrrolate or botulinum toxin on the hyperhidrotic segment, and she rejected these treatment options. Preventive measures and professional protections to avoid excessive body heat significantly improved her quality of life.
Fig. 1. Skin thermograms obtained using an infrared camera after 20 min exposure at 32°C, clearly delimited hyperhidrotic and anhydrotic areas (lower and higher estimated skin surface temperature respectively).
Discussion
The presence of segmental anhidrosis, tonic pupil (defined as a dilated pupil, constricting poorly to light and exhibiting near-light dissociation) and deep tendon hyporeflexia in our patient supported the clinical diagnosis of Ross syndrome. However, as reported in several studies, the main objective symptoms were the concomitant presence of a well-delimited compensatory hyperhidrosis and a disabling heat intolerance (1, 5, 6). Ross syndrome is considered as the expression of an unknown injury to the peripheral autonomic nervous system (7). Its exact pathogenesis is unknown. A wide overlap has been suggested between Ross syndrome, Holmes-Adie syndrome and more widespread autonomic disease (8). The sweating disturbance could result from a lesion of the sympathetic ganglion cells or their post-ganglionic projections. The hypothesis of a degenerative mechanism has recently been reported involving sudomotor fibres and other skin autonomic nerve fibres (innervating notably blood vessels and arrectores pilorum muscles) and, secondarily, other fibre types, such as epidermal sensory unmyelinated and myelinated fibres (1, 7). More recently, a direct infectious damage to autonomic nerves by an acute cytomegalovirus infection has been hypothesized in an isolated case report (3). Our patient experienced SS and had an auto-immune thyroid disease. To our knowledge Ross syndrome has not yet been associated with an autoimmune condition. SS is a systemic autoimmune disease characterized by Sicca symptoms, and accompanied by a wide variety of neurological complications, which can include autoimmune autonomic neuropathies (AAN) (9). A novel AAN entity characterized by positive ganglionic acetylcholine receptor (AChR) antibodies in the serum and designated autoimmune autonomic ganglionopathy (AAG) has been also been associated with SS (10). AAN and AAG are typically characterized by: (i) a diffuse autonomic failure (ileus, orthostatic hypotension, anhidrosis, reduced lacrimation, salivation and pupil constriction), that was not present in our case; and (ii) lack of compensatory hyperhidrosis. These considerations, associated with the fact that our patient had no serum AChR antibodies, led us to the final diagnosis of Ross syndrome. Our observation underlines the relevance of infrared thermography in the exploration of this thermoregulation disorder. This non-invasive examination permitted the direct observation of infrared body heat all over the skin surface at different ambient temperatures. It allowed us to validate, quantify and better localize the sweating and thermoregulatory abnormalities, and was thus clearly more efficient (and comfortable for the patient) than the classical Minor starch-iodine test. The infrared camera demonstrated an unexpected body “thermal pattern”, which might be highly evocative of Ross syndrome. To conclude, dermatologists must be aware of Ross syndrome, which may present as its main objective symptoms segmental hyperhidrosis and disabling heat intolerance. Although recent reports have linked certain dysautonomic syndromes with autoimmunity, this is the first report of a case of Ross syndrome associated with SS. Additional case reports are required to determine whether the association of these two conditions is causal.
The authors declare no conflict of interest.
References