Ágnes Kinyó1, Nóra Belső1, Nikoletta Nagy1, Attila Pálvölgyi2, István Nagy2, Irma Korom1, Erika Varga1, Lajos Kemény1 and Zsuzsanna Bata-Csörgő1
1Department of Dermatology and Allergology and 21st Department of Internal Medicine, University of Szeged, Korányi Str. 6, 6720 Szeged, Hungary. E-mail: kinyoagnes@gmail.com
Accepted September 10, 2010.
A relatively new drug used in the treatment of osteoporosis, strontium ranelate has been associated with several side effects, including increased relative risk of venous thromboembolism (including pulmonary embolism), transient increases in creatine kinase levels, mild gastrointestinal, nervous system and muscular disorders, and drug-induced hypersensitivity syndrome, also called DRESS syndrome (1). DRESS syndrome is a severe, acute drug reaction defined by the presence of fever, skin eruptions and systemic symptoms, including enlarged lymph nodes, abnormal liver function, renal impairment, and pulmonary and cardiac infiltrates, as well as haematological abnormalities, primarily hypereosinophilia and lymphocytosis (2, 3). We report here a case of a patient with strontium ranelate-induced DRESS who developed persistent autoimmune hepatitis.
CASE REPORT
A 69-year-old woman developed a skin rash with flu-like symptoms including fever (40°C) after taking strontium ranelate for four weeks. The strontium ranelate treatment was discontinued and methylprednisolone (16 mg/day) administered instead. After two weeks, and following a slight improvement in symptoms, steroid therapy was stopped. However, fever and generalised erythroderma developed again (Fig. 1). At this point, the patient was admitted to our clinic. Laboratory tests revealed the following: an erythrocyte sedimentation rate (ESR) of 11 mm/h (normal level < 20); a C-reactive protein (CRP) level of 55.6 mg/l (< 5); a white blood cell count of 16.47 × 109/l (3.9–11.1 × 109/l), of which 18 % were eosinophils (1.5–7.5%); thrombocytopenia (platelet count 137 × 109/l (169–358 × 109/l)); liver damage (glutamic-oxaloacetic transaminase (GOT) level 43 U/l (< 31), glutamic-pyruvic transaminase (GPT) level 60 U/l (< 31), alkaline phosphatase (ALP) level 326 U/l (< 240) and gamma-glutamyl transferase (GGT) level 128 U/l (< 32)); a normal serum bilirubin level; a serum carbamide level of 13.4 mmol/l (2.9–11.1); a serum creatinine level of 113 mmol/l (53–106); and proteinuria. The patient’s serum was negative for antinuclear antibodies (ANA). Analysis of a skin biopsy revealed extensive hydropic degeneration of basal keratinocytes, hyperkeratosis, granular spongiosis, keratinocyte necrosis and subepidermal eosinophilic infiltration. These findings were consistent with interface dermatitis seen in erythema exsudativum multiforme (Fig. 2). Based on these findings, we diagnosed DRESS. Methylprednisolone (125 mg/day) was administered intravenously for 4 days. The dose was then gradually tapered and the drug later replaced with prednisolone. The maintenance dose was 20 mg daily (at lower doses, the skin symptoms reappeared). The results of laboratory tests returned to normal. Two months later, the patient developed deep vein thrombosis. Acenocoumarol therapy was commenced, and her maintenance steroid therapy stopped. Her skin symptoms reappeared within a week of the steroid treatment being discontinued. Methylprednisolone treatment was reintroduced at a dose of 32 mg/day, and (tapered to 4 mg every second day). Three months later, the patient again stopped the steroid therapy. Shortly afterwards, a mild skin rash again developed on her arms and legs. Fresh laboratory tests revealed an ESR of 18 mm/h and a serum CRP level of 26.3 mg/l, and indicated serious liver damage (GOT level 468 U/l, GPT level 867 U/l, ALP level 327 U/l, GGT level 360 U/l, serum bilirubin level 22.1 mmol/l (< 19) and lactate dehydrogenase (LDH) level 613 U/l (< 530)). The patient’s serum was further found to be positive for ANA and smooth-muscle antigens (SMA). Serological tests (hepatitis B and C viruses, cytomegalovirus (CMV), Epstein-Barr virus (EBV), herpes simplex virus (HSV)-1 and HSV-2) were negative. Collectively, these results indicated the occurrence of autoimmune hepatitis. Low-dose prednisolone therapy was introduced again. The patient’s liver function test results improved 14 months after the initial appearance of DRESS. Presently she is taking prednisolone at a dose of 5 mg/day and her transaminase levels are normal.
Fig. 1. (A) Confluent maculopapular exanthema over the whole body. (B) Skin rash on the palm.
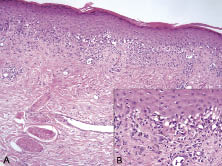
Fig. 2. (A) Histology of a maculopapular skin lesion, showing interface dermatitis (haematoxylin and eosin (HE) ×200). (B) Magnified image showing extensive hydropic degeneration of basal keratinocytes and subepidermal eosinophilic infiltration (HE ×400).
DISCUSSION
The most common triggering agents for DRESS are antiepileptic drugs, sulphonamides, antiretroviral drugs and allopurinol (4). Symptoms usually occur 2–6 weeks after the initiation of drug therapy. Often, discontinuation of the medication is insufficient to combat them, with systemic steroid therapy also being necessary. Symptoms can be long-lasting and require long periods of steroid treatment. Some manifestations may be life-threatening, with a mortality rate of 10% (5, 6). Genetic predisposition, altered drug metabolism and concurrent viral or bacterial infections are thought to contribute to disease induction. Skin symptoms – the result of a delayed-type hypersensitivity reaction – are almost always present and, although they show some variation in appearance, take the form of maculopapular rashes. In histology analyses, characteristic interface dermatitis – mononuclear cell infiltrate in the papillary dermis and basal keratinocyte necrosis – is observed at the dermo-epidermal junction: Moreover, the more basal keratinocyte cell death occurs, the more exfoliative the skin symptoms become, in severe cases resembling those associated with Stevens-Johnson syndrome and toxic epidermal necrolysis (7, 8).
To our knowledge this is the fifth reported case of DRESS syndrome associated with strontium ranelate. In one of the first two cases, the patient died of fulminant hepatitis linked to HHV6 virus reactivation, which was thought to have contributed to the development of DRESS syndrome (5). One case of bullous DRESS syndrome and one with renal failure have also been reported (9, 10). In our patient, autoimmune hepatitis was not related to reactivation of CMV, and serological tests for hepatitis B and C viruses, EBV, HSV-1 and HSV-2 were also negative (we did not test for HHV6 reactivation). Autoimmune hepatitis developed after she had been treated for deep vein thrombosis for several months with acenocoumarol. The hepatitis that initially occurred as part of the DRESS syndrome improved following steroid treatment. At that time, the results of ANA testing were negative. We did not initially test for other antibodies that are considered to be important in autoimmune hepatitis. Because coumarins are known to induce hepatitis, we cannot exclude the possibility that the long-lasting autoimmune hepatitis was caused by coumarin treatment. It is also possible that the two drugs, strontium ranelate and coumarin, together contributed to the development of liver disease. Because strontium ranelate increases the risk of thromboembolism, similar combined therapies are likely to be administered to other patients in the future.
The authors declare no conflict of interest.
REFERENCES