Charlotte Castronovo and Arjen F. Nikkels
Department of Dermatology, CHU du Sart Tilman, Liège University Hospital, Liège, Belgium



Charlotte Castronovo and Arjen F. Nikkels
Department of Dermatology, CHU du Sart Tilman, Liège University Hospital, Liège, Belgium
Although varicella zoster virus latency has been demonstrated in several sensory ganglia, herpes zoster usually effects only one single, either left or right, dermatome in half of the body. In immunocompromised patients, more than one contiguous unilateral dermatome may be involved. Bilateral non-contiguous herpes zoster, also termed herpes zoster duplex, is rarely reported. Chronic varicella zoster virus skin infection is another rare entity encountered in HIV-infected and immunocompromised patients, often associated with aciclovir resistance. We describe here a patient with chronic lymphocytic leukaemia, who presented simultaneously non-contiguous bilateral and chronic herpes zoster lasting for more than 2 months, with resistance to aciclovir. To our knowledge, this is the first report of chronic herpes zoster duplex bilateralis. Physicians should be aware of and recognize these atypical manifestations of varicella zoster virus. Key words: herpes zoster; varicella zoster virus; immunosuppression.
(Accepted May 4, 2011.)
Acta Derm Venereol 2011; 91: XX–XX.
Arjen F. Nikkels, Department of Dermatology, University Medical Center of Liège, BE-4000 Liège, Belgium. E-mail: af.nikkels@chu.ulg.ac.be
Following varicella, the varicella zoster virus (VZV) remains dormant in the sensory dorsal root ganglia (1–3). After reactivation, viral replication produces virions that travel to the skin, along the axonal microtubular system, producing the typical unilateral herpes zoster (HZ) lesions, usually restricted to a part of a dermatome (2). Sometimes, HZ can affect more than one dermatome, in particular in the immunocompromised individual, termed multidermatomal HZ (2, 4). Usually, the involved dermatomes are contiguous and unilateral (2, 4). HZ duplex unilateralis or bilateralis, concerning two non-contiguous and widely separated dermatomes, is even less common (4, 5). Longstanding or chronic VZV skin infections are another rare manifestation (6). They are usually reported in HIV-infected and immunocompromised individuals, and are often associated with aciclovir resistance (6).
To our knowledge, this case report is the first of a patient presenting HZ duplex bilateralis simultaneously with a longstanding disease course and aciclovir-resistance.
Case report
A 70-year-old Caucasian man was diagnosed with chronic lymphocytic leukaemia (CLL) Binet grade B in 2003. Initial therapy consisted of chlorambucil and methylprednisolone. As there was no response, the patient was treated with 4 courses of fludarabine 40 mg/m2 /day, with good clinical response. In 2006, a recurrence of CLL was treated with chlorambucil 5 mg/day. In 2009, bone marrow infiltration by a small cell lymphoma was observed. A biopsy from a lymphatic ganglion revealed CD5+ small cell CLL, IgM kappa+ and a large proliferative centre. Proliferation estimated by Ki67 immunostaining was < 20%. An aggressive transformation of the CLL was diagnosed (Richter syndrome). The patient developed HZ, simultaneously affecting the right C4, T2 dermatomes (Fig. 1) and the left L 1,2 dermatomes (Fig. 2). A major part of the dermatomes was affected. The lesions consisted of a small erythematous base with central vesiculation. Some lesions were pustular. Previously, the patient presented prodromal pains in the areas of skin involvement. The patient had no lymphadenopathies, fever or headache. A skin biopsy revealed intra-epidermal vesiculation with giant multinucleated cells and intranuclear inclusions, suggestive of an alpha-herpesvirus infection. Immunostainings with anti-VZV (anti-gE) (7), anti-HSV-I and anti-HSV-II antibodies (Dakopatts, Denmark) revealed positive marking for VZV (Fig. 3), whereas both anti-HSV antibodies were negative. Intravenous Aciclovir was initiated at 10 mg/kg/8 h. The vesicular and pustular lesions diminished, but, despite treatment, there was still no complete resolution after 15 days. A new skin biopsy still demonstrated positive VZV immunostaining. As no new vesicles developed, the patient was dismissed with oral aciclovir 800 mg 5 times/day. Two months later, the patient was again referred to the dermatology department. Clinical examination revealed a similar eruption to the one seen previously, affecting the same dermatomes. Additionally, he presented some satellite lesions beyond the previously involved dermatomes (Figs 1, 2). As aciclovir-resistance was suspected, the patient was hospitalized for intravenous aciclovir treatment at 10 mg/kg/8 h, or intravenous foscarnet. A viral culture for aciclovir-susceptibility testing was not performed, as the patient’s general status deteriorated rapidly. A left basal bronchopneumonia developed with Staphylococcus aureus sepsis. Despite adequate intravenous antibiotherapy and supportive treatment, the patient died. Permission for autopsy was denied.

Fig. 1. Chronic herpes zoster duplex bilateralis of the right C4, T2 dermatomes.

Fig. 2. Chronic herpes zoster duplex bilateralis of the left L 1, 2 dermatomes in the same patient.
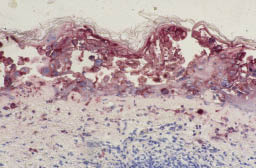
Fig. 3. Immunohistochemical staining (red signal, Fast Red) revealing the varicella zoster virus (VZV)-gE protein in infected keratinocytes (× 100, Mayer’s hemalun).
Discussion
As far as we know, this is the first report of chronic HZ duplex bilateralis with aciclovir-resistance in an immunocompromised patient. Until now, only 23 cases of HZ duplex unilateralis or bilateralis have been reported (8–29). The incidence of HZ duplex bilateralis was estimated below 0.5% (16), but is probably much lower. Table I summarizes the ethnicity, age and gender, involved dermatomes, the presence of satellite lesions, the medication, the underlying illness, the diagnostic methods, the treatment and whether post-herpetic neuralgia was observed, for the 23 reported cases of HZ duplex. HZ duplex was observed in all ethnic groups, but the high number of patients of the Far East may suggest a genetic susceptibility for developing HZ duplex. The mean age of the patients was 44.4 years (age range 3–77 years). There were 13 women and 10 men. The majority of the adult and paediatric cases had immunosuppression, leukaemia and lymphoma in particular. The most frequently involved areas were the thoracic dermatomes, followed by the cervical and trigeminal dermatomes. Contiguous multidermatomal involvement was common. Disseminated satellite lesions beyond the dermatomes were found in 5/23 cases as well as in our patient. Clinical diagnosis was usually confirmed by a Tzanck smear or a skin biopsy. Viral culture and PCR were only seldom used. Antiviral treatment with aciclovir or FCV was most often initiated. Curiously, several cases were treated with oral antivirals, despite the immunosuppressed status of the patients. Underdosing was common with regard to dosing recommendations. No cases presented signs of internal VZV dissemination or other complications. PHN was recorded in 2/23 patients. One patient presented motor deficiencies without cutaneous involvement (22). One patient presented recurrent episodes of HZ duplex (13). In one child with HZ duplex, satellite VZV lesions continued to appear for a month (20). Interestingly, in two cases, restriction endonuclease analysis demonstrated that the virus strain isolated from two distinct dermatomes was identical (19, 29).
Table I. Overview of reported cases of herpes zoster (HZ) duplex
| Origin | Age, years/sex | Dermatomes | Satellite VZV | Medication | Underlying disease | Diagnosis | Treatment | Ref. | |
| 1 | Arabic | 64/F | L: T8 R: L4 | – | Prednisone | Polymyositis Diabetes | Clin | IV ACV 30mg/kg/day 15d, no PHN | 8 |
| 2 | Korean | 67/F | L: T7,8 R: L4,5 | – | ? | Hypertension Osteoporosis | Tz Biop | FCV 750mg/day 1 week No PHN | 9 |
| 3 | Korean | 49/F | L: T4 R: T4 | – | 5-fluorouracil Methotrexate Adriamycin. | Breast cancer | Tz Biop PCR | FCV 750mg/day 1 week No PHN | 10 |
| 4 | Hungary | 73/F | L: T9,10 R: L2,3, S3 | – | / | / | Cult | Isoprinosine 4×1g/day, 14 day no PHN | 11 |
| 5 | Japan | 72/F | L: facial paresis R: peroneal paresis | – | ? | Diabetes | ? | ? | 12 |
| 6 | Indian | 30/M | L: T10 R: T10 | – | ? | HIV | Tz | ? | 13 |
| 7 | Indian | 24/F | L: eye R: tigh | – | / | / | Tz Biop | Oral ACV 5×/day 10 day No PHN | 14 |
| 8 | Indian | 10/M | L: L 2–4 R: C4–6 | – | ? | HIV Haemophilia | IV ACV, 10 mg/kg/8 h, 7day | 15 | |
| 9 | Indian | 50/M | L: C3–5 L: T7–9 | – | Immunosuppressive drugs | Renal transplant | IVACV, 10 mg/day/ 8 h, 9 day PHN | 15 | |
| 10 | American | 69/M | R: T5–7, 10,12, L3–4 L: T4–6,1, L3–5 | + | Cyclosporine Prednisone Mycophenolate | Renal allograft | DIF Tz Cult | IV ACV 800 mg/day for 7 day oral FCV 500 mg/day 14 day | 16 |
| 11 | Caucasian | 67/M | R: V3 L: V1,2 | – | Oral steroids | / | Biop | ACV 200 mg 5×/day, 5 day No PHN | 17 |
| 12 | Chinese | 52/F | R: T2,3 L: T8 | – | Oral steroids | Systemic lupus | Biop | / scarring, no PHN | 18 |
| 13 | Japan | 3/F | R: T2–4 L: T2–4 | + | Chemotherapy | Lymphocytic leukaemia | ACV IV 5 mg/kg/8 h | 19 | |
| 14 | American | 10/M | R: V, T4 L: T2 | + | Steroids, chemotherapy | Non-Hodgkin’s lymphoma | Cult | VZV Immunoglobulins | 20 |
| 15 | Caucasian | 16/F | R: V2 L: T4–7 | – | / | / | Clin | ACV IV 500 mg 3×/j 8 day | 21 |
| 16 | Korean | 5/F | R: T5 L: T2 | – | / | / | Tz Biop | ACV No PHN | 22 |
| 17 | Korean | 22/F | R: T7 L: S3 | – | Chemotherapy | Leukaemia | Tz | FCV 750 mg/day 7 day No PHN | 23 |
| 18 | Korean | 47/F | R: T7 L: L3,4 | – | / | / | Tz Biop | ACV IV No PHN | 24 |
| 19 | Pakistan | 24/M | R: T8 L: T8 | + | / | / | Tz Biop | ACV oral 800 mg 5×/day 7day | 25 |
| 20 | Scot | 76/F | R: V1 L: V3 | – | / | / | Clin | ACV oral 200 mg 5×/day No PHN | 26 |
| 21 | Korean | 76/M | R: V1 R: L1,2 | + | ? | COPD | Tz Biop | ? | 27 |
| 22 | American | 37/F | R: T3 L: T11 | – | Oral steroids | Asthma | Clin | ACV oral | 28 |
| 23 | Japan | 77/M | R: T6–8 L: S3,4 | – | ? | Gastric cancer | ? | ? | 29 |
M: male; F: female; Y: year; L: left; R: right; C: cervical; T: thoracic; L: lumbar; S: sacral; Diag: diagnostic method; VZV: varicella zoster virus; lesions COPD: chronic obstructive pulmonary disease; DIF: direct immunofluorescence; Clin: clinical examination; Biop: skin biopsy; Cult: viral culture; Tz: Tzanck smear; IV: intravenous; ACV: aciclovir; FCV: famciclovir; PHN: post-herpetic neuralgia.
HZ duplex is the ultimate clinical proof that VZV remains latent in the majority of sensory dorsal root ganglias, as has been previously suggested by the demonstration of VZV DNA in trigeminal, cervical, thoracic, lumbar and sacral dorsal root ganglias in autopsy studies (3, 30). The reason why viral reactivation leads to only a single unilateral dermatomal HZ eruption is probably related to the quantity of VZV viral genome load distribution in the different dorsal root ganglias (31). It is hypothesized that the highest viral genome load leads to clinical HZ (31). Concurrent VZV-specific immunoboosting induced by the HZ eruption probably avoids other eventual reactivations to become clinical. Only in cases of severe immunosuppression, VZV can be reactivated in multiple dorsal root ganglias and conduct to multidermatomal HZ can be involved. The satellite lesions are probably of haematogenous origin (32).
The HZ duplex persisted for more than 2 months and did not respond to aciclovir oral or intravenous therapy. These features are indicative for chronic VZV skin infection with aciclovir-resistance (6), although there was no formal proof. Aciclovir resistance for VZV is almost non-existent in immunocompetent individuals, but is not uncommon in immunocompromised patients. Chronic VZV skin infections are observed in HIV patients receiving highly active antiretroviral therapy (HAART) and immunocompromised patients (6). They have an indolent character and present no risk for internal viral dissemination (6). In the case of aciclovir-resistance by thymidine kinase deficiency or a truncated protein, intravenous foscarnet would have been the first alternative antiviral as it is not thymidine kinase dependent (6). Another explanation for the chronic disease course may be the general immunodeficient state of the patient.
In conclusion, HZ duplex unilateralis or bilateralis is a rare event. It is almost exclusively restricted to the immunocompromised patient. It seems, however, not to represent a risk factor for poor prognosis. Chronic evolution is possible. This first case of chronic HZ duplex bilateralis enriches the ever-expanding spectrum of VZV-associated skin manifestations.
References

