A. Tulin Mansur1 and Ikbal E. Aydingoz2
1Dermatology Clinic, Ahu Hetman Hospital, Marmaris, Mugla, and 2Department of Dermatology, Acibadem University School of Medicine, Istanbul, Turkey. E-mail: tulinmansur@hotmail.com
Accepted June 7, 2011.



A. Tulin Mansur1 and Ikbal E. Aydingoz2
1Dermatology Clinic, Ahu Hetman Hospital, Marmaris, Mugla, and 2Department of Dermatology, Acibadem University School of Medicine, Istanbul, Turkey. E-mail: tulinmansur@hotmail.com
Accepted June 7, 2011.
Fordyce spots (FS) are ectopic sebaceous glands clinically characterized by minute orange or yellowish pinhead-sized macules or papules located in different sites in the oral cavity, mainly at the upper lip vermilion, retromolar area, and buccal mucosa. In most cases the clinical features are characteristic enough to diagnose FS easily without the need for histopathological examination (1).
We report here a patient with unilateral, intraoral FS, and ipsilateral facial paralysis.
CASE REPORT
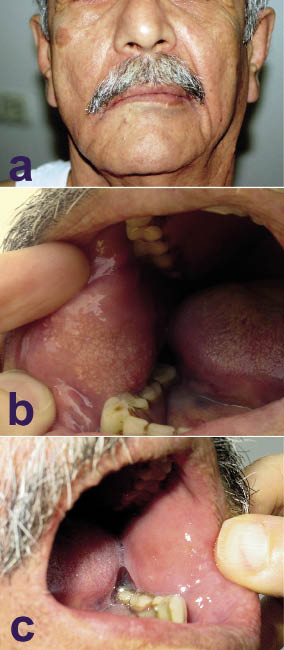
A 58-year-old man was referred for a routine skin examination. His medical history revealed a right-sided facial paralysis that had occurred 10 years previously, in the absence of any identifiable cause. After treatment, he had incomplete recovery with considerable sequelae of facial paralysis, including facial asymmetry and limited masticator function of the involved area. Physical examination revealed obvious weakness of the buccal muscles, with loss of facial creases and nasolabial fold, dropping of the corner of the mouth, and mild weakness of eye closure on the paralysed side (Fig. 1a). Oral mucosal examination showed closely-grouped asymptomatic yellow maculopapules, 1–2 mm in diameter, on the right buccal mucosa, which were clinically consistent with FS (Fig. 1b). The appearance of the left buccal mucosa was normal (Fig. 1c).
Fig. 1. (a) Typical clinical findings of the right-sided facial paralysis. (b) Right buccal mucosa studded with tiny, yellow maculopapules. (c) Normal mucosa of the left cheek.
DISCUSSION
FS present simply as ectopic variants of normal sebaceous glands. The only difference between FS and ordinary sebaceous glands is that they lack an association with the hair follicles and have ducts opening directly onto the skin surface. These lesions affect both genders, and usually become prevalent after puberty, most probably due to hormonal changes stimulating the enlargement of sebaceous glands. The lesions are normally bilateral and rather symmetrical (1). Unilateral FS of the oral mucosa have not been reported previously. The case described here is interesting for the restriction of FS to the side of facial paralysis. It is not clear whether this is a coincidence or a true relationship. The patient could not provide the chronological information about the development of FS, i.e. before or after the facial paralysis. Nevertheless, the asymmetrical involvement of the paralytic site and the unusual concentration of the lesions in this location require explanation.
There are some early reports documenting the close interactions between human sebaceous glands and the neurological system. Bettley & Marten (2) were the first authors to describe the development of unilateral facial seborrhoea and seborrhoeic dermatitis after facial nerve paralysis.
In fact, facial nerve supplies all the muscles of facial expression and provides parasympathetic and sympathetic fibres to the lacrimal glands and parasympathetic fibres to the salivary glands (3). Contrary to expectations, innervation of facial skin is mainly through the trigeminal nerve. The buccal nerve, which is a small branch of the mandibular division of the trigeminal nerve, also supplies the cheek mucosa. However, it has been shown that there are several communicating branches between the buccal nerve and the facial nerve (4). Hence, facial nerve paralysis may exert functional effects on the cheek mucosa.
For the presented case, the mediators that stimulate axonal regeneration may have played a role in the stimulation of sebaceous glands and the development of FS. Peripheral nerve injury is known to induce changes in neuropeptides, signal transduction molecules, and growth-associated proteins/neurotrophic factors, which may be due to injury itself, or the altered environment brought about by the regenerating axons (5, 6). Though the repair process was not successful in our patient, we can at least assume that the regeneration system should have worked to a certain extent.
In normal facial skin it has been generally accepted that sebaceous glands are not innervated and are not affected by the peripheral nervous system. However, in recent years some investigations have denoted the interaction between neurological system and sebaceous glands. Human sebocytes express receptors for neurotransmitters, which are mostly arranged on the cell surface (7). Nerve growth factor (NGF) is an essential neuromediator, which plays an important role in peripheral axonal regeneration, promoting the sprouting of nerve fibres (8). Specifically, it has been reported that P75 NGF receptor is expressed in regenerating human facial nerve grafts (9). Prominent expression of NGF and its receptors in sebaceous glands of healthy scalp skin have been shown (8). Germinative cells, which are the outermost layer of the sebaceous acini also express high levels of NGF in patients with acne (10). Moreover, in facial skin of patients with acne, numerous fine nerve fibres have been found around and within sebaceous acini (10). Vasoactive intestinal peptide and calcitonin gene-related polypeptide are other neuromediators that are induced strongly after neuronal injury and believed to mediate neuroregenerative actions (5, 6). It is also known that these neuropeptides have receptors to bind human sebocytes and stimulate their proliferation and differentiation (7). Furthermore, IGF-1, a common growth factor that promotes nerve elongation and branching has been shown to have a potent effect on proliferation of the preputial sebaceous glands, which are counterpart to FS (11, 12). Corticotrophin-releasing hormone (CRH) is another important mediator that has been shown to have a role in nerve regeneration via facilitating axon outgrowth (13). The receptors for this mediator are also expressed on the sebocytes, and after CRH binding they modulate differentiation and lipogenesis of sebocytes (14). Therefore, it may be speculated that the increased secretion of CRH in the injured nerve may have stimulated the ectopic sebaceous glands of buccal mucosa. Another way of thinking is that the sebaceous hyperplasia may be a consequence of an attempt of the body to repair the injured nerve, since basal and differentiating sebocytes have been shown to demonstrate a strong positive reaction for CRH (14).
Finally, some other factors related to facial paralysis may also have contributed to the asymmetrical involvement of FS. Chronic nerve inactivity, resultant muscle paralysis, reduction of salivary flow, repeated cheek biting on the paralysed side, and all the complex interactions taking place in this microenvironment may also have been involved. To the best of our knowledge, there is no previous study investigating the effects of mechanical injury on the functions of sebaceous glands.
In conclusion, the case described here may support a causal relationship between the hyperplasia of sebaceous glands and facial paralysis. This observation provides further information about the functioning of human sebaceous glands within the nervous system as a target organ.
REFERENCES

