Thomas Volz1, Florian Wölbing1, Jörg Fischer1, Martin Braun2, Iryna Maggoschitz2, Martin Schaller1, Mark Berneburg1 and Tilo Biedermann1
1Department of Dermatology, Eberhard Karls University, Liebermeisterstrasse 25, DE-72076 Tübingen and 2Dermatology practice Dr M. Braun, Überlingen, Germany. E-mail: tilo.biedermann@med.uni-tuebingen.de
Accepted October 19, 2011.
Schnitzler syndrome is a rare disease presenting with chronic urticaria and monoclonal gammopathy. Its pathogenesis is unclear and therapies effective in chronic urticaria remained without effect (1, 2). However, whether systemic or cutaneous IL-1 elicits urticaria in these patients is not known, because the source of IL-1 remained enigmatic. Here we demonstrate for the first time the presence of active IL-1β by immunohistochemistry in dermal cells of affected skin in a patient with Schnitzler syndrome. This not only underlines the rationale to treat Schnitzler syndrome with IL-1 blocking agents; it also demonstrates that immunoglobulin M (IgM), or yet unknown factors associated with monoclonal gammopathy in these patients, trigger IL-1 activation also in the skin, as gene defects do in patients with Muckle-Wells (MWS) or cryopyrin-associated periodic syndroms (CAPS) (3, 4). Consequently, treatment with the IL-1 receptor antagonist (IL-1RA) anakinra, initiated as first-line monotherapy, led to complete remission of symptoms within 2 days, and long-lasting remission for more than 3 years was achieved by daily administration of anakinra.
CASE REPORT
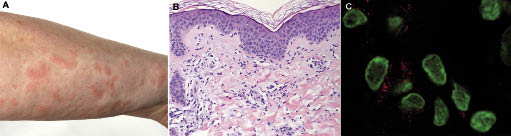
A 59-year-old woman presented with a 5-year-history of daily episodes of urticaria. Wheals were located at the trunk, the upper limbs and the thighs and were accompanied by musculoskeletal and bone pain as well as by attacks of fever. In contrast to patients with chronic urticaria, wheals never elicited itch, and therapies with high-dose antihistamines had no effect. Upon physical examination generalized urticaria was documented (Fig. 1A). Histological analysis of wheals revealed a sparse infiltrate of neutrophils devoid of leukocytoclasia compatible with the diagnosis urticaria without signs of vasculitis (Fig. 1B). Importantly, immunohistochemistry performed from specimens of affected skin revealed dermal expression of active IL-1β, as shown by staining with a monoclonal antibody recognizing cleaved IL-1β (Fig. 1C), whereas cleaved IL-1β was absent in control skin (not shown). Laboratory investigations showed leukocytosis (10.94 × 109/l), elevated erythrocyte sedimentation rate of 53 mm/h and increased C-reactive protein (CRP) (57.5 mg/l). Increased IgM levels (516 mg/l) were detected, while serum levels for IgG and IgA were normal. In addition, elevated levels of free kappa light chains (51.1 mg/l) were detected and immunofixation confirmed a monoclonal gammopathy of the IgM type. No lymphoproliferative disorder could be detected in the bone marrow biopsy. Ultrasound revealed a mild splenomegaly without hepatomegaly and peripheral lymphadenopathy. Arthritis was ruled out by 3-phase-scintigraphy.
Based on the clinical and laboratory findings, the diagnosis of Schnitzler syndrome was made. Given the observed IL-1β expression in affected skin lesions, and recent reports on patients with Schnitzler syndrome that failed to respond to any other treatment but the use of the IL-1RA anakinra, prompted us to administer anakinra as first-line therapy. Subcutaneous injection of 100 mg anakinra per day was started, and within 48 h a complete and sustained remission of the urticarial rash occurred (Fig. 2A), while the patient noticed the disappearance of musculoskeletal pain and arthralgias. Leukocyte counts rapidly normalized, and elevated C-reactive protein levels constantly decreased within the first 3 days after onset of therapy (Fig. 2B). Monotherapy with anakinra 100 mg daily was continued in the absence of any side-effects for more than 3 years, and the patient is still in complete remission.
Fig. 1. Schnitzler syndrome presenting with urticaria and dermal interleukin (IL)-1β expression. (A) Generalized urticaria affecting the trunk and the upper limbs. (B) Histological analysis of wheals with a sparse infiltrate of neutrophils devoid of leukocytoclasia. (C) Immunohistochemistry with a monoclonal antibody (mAb) against mature IL-1β reveals dermal expression of active IL-1β (red). Nuclei are stained green with YoPro dye.
Fig. 2. Rapid clearance of symptoms in Schnitzler syndrome in response to anakinra. (A) Complete clearance of urticaria within 48 h after onset of anakinra therapy. (B) Normalization of leukocyte count and elevated C-reactive protein levels within the first 3 days of anakinra treatment.
DISCUSSION
Schnitzler syndrome typically presents with non-itching urticaria that is unresponsive to even high-dose antihistamines. The diagnosis of Schnitzler syndrome can be considered on the basis of the 2 major criteria:”chronic urticarial rash” and “monoclonal gammopathy” in combination with at least 2 minor criteria as reviewed by Lipsker et al. (1) and de Koning et al. (2). Exclusion of haematological malignant diseases and other autoimmune disorders is mandatory.
The pathogenesis of the symptoms in Schnitzler syndrome is still unknown. Interestingly, excessive secretion of IL-1, IL-6 and tumour necrosis factor (TNF) after lipopolysaccharide stimulation of peripheral blood mononuclear cells from patients with Schnitzler syndrome has been demonstrated, and only administration of a caspase inhibitor reduced IL-1 secretion, while blocking TNFα had no effect (5). Together with our new findings of dermal expression of active IL-1β this points to a central role of the inflammasome-controlled IL-1 production as a crucial step in its pathophysiology. The best evidence that Schnitzler syndrome is a disease of exaggerated IL-1 activation is the successful use of the IL-1RA anakinra in its treatment (2, 6, 7). Anakinra is the first drug that effectively treats Schnitzler syndrome without detectable side-effects. Treatment of Schnitzler syndrome has been difficult as non-steroidal anti-inflammatory drugs, systemic steroids methotrexate, azathioprine or cyclosporine were not effective. Confirming observations by others, the IL-1RA anakinra, within hours to days after onset of therapy, completely resolved disease symptoms in our patient. Urticaria is the dominant finding in Schnitzler syndrome, but it is not known whether urticaria develops as a consequence of systemic IL-1 levels or as a consequence of cutaneous IL-1 activation. Immunohistochemistry with the detection of active IL-1β in skin cells of our patient is the first indicator of cutaneous IL-1 activation in this disease. Thus, unknown factors associated with monoclonal gammopathy are capable of eliciting peripheral IL-1 activation. This finding in Schnitzler syndrome is similar to inherited diseases with excessive IL-1 activation, such as CAPS, MWS or familial cold urticaria, in which IL-1 activation is also found in the skin (8, 9). Detection of cleaved IL-1β in the skin may help to distinguish urticaria in Schnitzler syndrome from other forms of urticaria, as we could not detect IL-1β in specimens from patients with chronic idiopathic urticaria (data not shown). Clinical improvement was accompanied by declining leukocyte counts and CRP levels within a few days demonstrating the systemic effects of IL-1R blockade. Full remission lasting for more than 3 years was achieved by continuous therapy with daily subcutaneous injections. To our knowledge this is also the first report demonstrating such long-lasting improvement of Schnitzler syndrome by monotherapy with anakinra in the absence of any side-effects.
Although Schnitzler syndrome has a benign course, development of Waldenström’s macroglobulinaemia has been reported (2). Thus, long-term follow-up is necessary to detect development of haematological malignancies. Whether therapy with anakinra or newly developed IL-1 blocking drugs (Rilonacept or Canakinumab) may decrease the risk of developing haematological malignancies due to an ongoing inflammatory immune response has to be evaluated. Taken together, administration of the IL-1RA anakinra has emerged as an effective treatment for the still enigmatic Schnitzler syndrome and should be the therapy of choice in newly diagnosed patients.
REFERENCES