Patients who have received liver transplant are at increased risk of skin complications due to long-term immunosuppression regimen. The aim of this study was to analyze the incidence and risk factors of skin complications in liver transplant patients. We analyzed 161 liver transplant recipients. The mean age at transplantation was 47.4 years. Mean follow-up was 6 years. Seventy-one percent of patients presented with skin complications, including aestethic alterations, infections, precancerous lesions and malignancies, which represented 57%, 43%, 18% and 9%, respectively. Risk factors were: age at transplantation ≥ 45 years, immunosuppressive therapy with cyclosporine, and phototype II and III. Our study indicates that although liver transplant recipients are at greater risk of developing skin complications compared to the general population, the risk is lower than for other solid organ transplants, particularly for premalignant and malignant lesions. Key words: cutaneous diseases; cyclosporine; tacrolimus; skin cancer; liver transplant.
(Accepted November 28, 2011.)
Acta Derm Venereol 2012; 92: XX–XX
Mauro Alaibac, MD, PhD, Unit of Dermatology, University of Padua, Via C.Battisti 206, IT-35128 Padova, Italy. E-mail: mauro.alaibac@unipd.it
Liver transplantation is often the only remaining therapy for patients with end stage liver cirrhosis, acute liver failure and some metabolic and congenital hepatic diseases. Advances in surgical techniques, the availability of more efficacious immunosuppressive regimens, and dedicated transplant units, have led to an extended life for liver transplant recipients (LTRs) (1). This longer-living transplant population may exhibit cutaneous complications, some of which may lead to death whilst others lead to a decline in the quality of life (2).
Several factors are known to predict skin complications in LTRs, notably long-term immunosuppressive regimen, age, sex, phototype, sun exposure, viral infections, and individual genetic characteristics (2, 3).
While cutaneous alterations have been extensively studied in kidney and heart transplant recipients, reports on LTRs are infrequent (4–6). With regard to the development of skin cancer and other cutaneous complications, LTRs seem to have a lower incidence of skin carcinomas and a higher number of Kaposi’s sarcoma compared to other organ transplant recipients (7, 8).
The aim of this study was to analyze the incidence and risk factors of skin complications in LTRs with particular reference to skin malignancies.
METHODS
Patients
We included LTRs followed-up both at the Unit of Gastroenterology and at the Unit of Dermatology of the University of Padua. Data were analyzed from a prospective cohort study of 161 adult LTRs who received their first liver transplant between December 1987 and August 2006. Our patients had a follow-up of at least one year and all subjects underwent a full skin examination by a dermatologist every 6 months. The frequency of follow-up dermatological visits was increased to every 3 months when a malignant or premalignant skin lesion was diagnosed. All patients were given a questionnaire about risk factors for skin complications, notably age, sex, sun exposure (sun exposure during holidays and occupational sun exposure categorized in 2 groups: yes versus no), primary liver disease, family history of skin neoplasms or other malignancies, diet, history of smoking or alcohol consumption.
Immunosuppressive regimen
All patients were strictly followed-up by hepatologists who prescribed the proper immunosuppressive regimen. We divided patients on the basis of the primary immunosuppressive therapy (cyclosporine or tacrolimus) and the secondary immunosuppressant, if needed (mycophenolate mofetil or azathioprine). All patients received steroid induction therapy which was gradually tapered over a period of 3–6 months, with the exception of 4 patients transplanted for autoimmune hepatitis who continued to receive steroid treatment. Acute rejection therapy consisted of 1–3 boluses of 1 g of methylprednisolone.
Statistical analysis
Data were collected using a Microsoft Excel 2003 database and statistical analyses were performed using the SAS software package. Results were expressed as mean ± standard deviation unless otherwise specified. A comparison of mean values was made by Student’s t-test. The ordinal data were analyzed using the Pearson’s chi-squared test and Fisher’s exact test. The risk of developing each type of skin complication after liver transplantation was evaluated using the density incidence and the crude cumulative incidence. The risk of developing skin diseases after transplantation was evaluated using the Kaplan-Meier survival analysis. Outcomes in the analysis included time of diagnosis of skin diseases or the date of patient’s death. Multiple logistic regression models were applied to evaluate the potential association of individual factors with the development of skin complications. The explanatory variables included in the multiple logistic regression models were the following: sex, age at transplantation, type of immunosuppressive therapy, acute rejection, sun exposure (before liver transplantation and after liver transplantation, exposure during the holidays and occupational exposure), cause of liver failure, family history of skin neoplasms or other malignancies, presence of warts or actinic keratosis. A p-value < 0.05 was considered significant.
RESULTS
General features
The transplant population consisted of 116 men and 45 women. The mean age at transplantation was 47.4 ± 11.0 years. Thirty-one patients (19%) were followed-up for longer than 10 years, 44 (27%) for 7–10 years, 25 (16%) for 5–7 years, 30 (19%) for 3–5 years and 31 (19%) for 1–3 years. The mean observation period was 6 years. Seven patients (4.35%) died during the follow-up period.
The indications for liver transplantation were as follows: 52 (32.3%) hepatitis C virus (HCV)-related cirrhosis, 32 (19.9%) alcohol-related cirrhosis, 27 (16.8%) hepatitis B virus (HBV)-related cirrhosis with or without hepatitis D virus (HDV) co-infection or super-infection, 9 (5.6%) HBV-HCV-related cirrhosis, 5 (3.1%) hepatocellular carcinoma (HCC), 36 (22.3%) other liver diseases (primary biliary cirrhosis, autoimmune hepatitis, Budd-Chiari syndrome, cryptogenic cirrhosis, Caroli syndrome, Wilson disease, hemochromatosis, 1-alpha 1-antitrypsin deficiency, hepatic fibrosis, neuroendocrine neoplasia, acute liver failure).
None of the patients were phototype I or VI. Therefore we divided patients in 2 groups according to their phototype: one group with skin phototype II/III (85 patients, 52.8%) and the other group with skin phototype IV/V (76 patients, 47.2%).
A family history of skin cancer was found in 5 patients (3.1%) whereas 57 (35.4%) reported at least one case of non-cutaneous neoplasm in their family. Eighty-seven patients (54%) had a history of smoking before transplantation.
Cutaneous complications
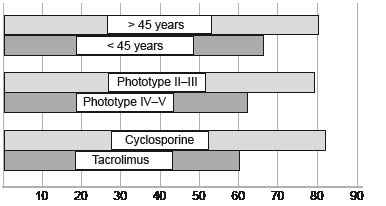
One hundred and fourteen out of 161 patients (71%) presented skin complications: 69 (43%) showed infective complications, 92 (57%) aesthetic complications, 29 (18%) pre-neoplastic complications and 14 (9%) neoplastic complications (Table I). Among these 114 patients, 49 (30.4%) developed only one type of cutaneous complication, 45 (28%) 2 types, 14 (8.7%) 3 types and 6 patients (3.7%) developed all 4 types of skin complications. We observed a statistically significant association between the development of skin complications and the primary immunosuppressive therapy regimen; crude cumulative incidence of a single complication was 81.8% in patients using cyclosporine and 59.7% in patients using tacrolimus (p = 0.003). In this group of patients, crude cumulative incidence was 78.8% in patients with phototype II–III and 61.8% in patients with phototype IV–V (p = 0.018). Moreover, dividing patients with skin complications into 2 subcategories according to age (< 45 years old and ≥ 45 years old), patients ≥ 45 years developed cutaneous complications more frequently as compared to patients < 45 years (80.4% versus 66.3%; p = 0.06) (Fig. 1). In the group of patients with more than one cutaneous complication, crude cumulative incidence was statistically higher in patients using cyclosporine versus patients using tacrolimus (p = 0.02) and in patients with phototype II–III versus patients showing phototype IV (p = 0.016). Therefore, major risk factors for cutaneous complications were a cyclosporine-based immunosuppressive regimen and a skin phototype II–III; a total of 34 (23%) patients having both these risk factors were identified, and the crude cumulative incidence for any type of cutaneous complication in these 34 patients was 94% versus 64.6% of the other patients (p = 0.001).
Table I. Prevalence of skin complications in the population of liver transplant recipients according to time after transplantation.
| | < 1 years n (%) | 2–3 years n (%) | 3–5 years n (%) | > 5 years n (%) |
| All | 15 (45) | 24 (54) | 34 (80) | 88 (100) |
| Infectious | 2 (13) | 2 (8) | 13 (38) | 52 (59) |
| Aesthetic | 3 (20) | 10 (42) | 15 (44) | 64 (73) |
| Preneoplastic | (0) | 1 (5) | 4 (12) | 24 (27) |
| Neoplastic | (0) | (0) | 3 (9) | 11 (12) |
Fig. 1. Crude cumulative incidence (%) of skin complications (all types) observed in the different groups of patients. p-values for the different groups: cyclosporine/tacrolimus: p = 0.003, phototype II–III/IV–V: p = 0.018; older/younger than 45 years: p = 0.06.
Multiple logistic regression analysis showed that development of skin complications was mainly related to the use of cyclosporine as the primary immunosuppressive agent; patients undergoing a cyclosporine-based immunosuppression had a risk of skin complications which was 3 times higher than that of tacrolimus-treated patients (odds ratio (OR) 2.9, 95% confidence interval (CI) 1.3–6.4).
Infectious complications
Forty-three percent (crude cumulative incidence) of patients developed an infectious cutaneous disease, including viral warts, superficial mycoses, deep mycoses, bacterial infections, and herpetic infections, with an incidence density of 9.4% person-year (Table II). The most frequent infectious cutaneous complication was the development of viral warts; the mean time of development was 3.1 years, and the medium-time survival was 15.2 years (95% CI 12.6–15.3) after diagnosis was established. The development of viral warts was statistically related to a cyclosporine-based immunosuppressive regimen (OR 2.67; 95% CI 1.13–6.3). None of the other variables analyzed in our study were statistically associated with infectious cutaneous complications.
Table II. List of infectious complications observed in the patients.
| Infectious complications | Patients affected n (%) |
| Warts | 30 (19) |
| Mycotic intertrigo | 21 (13) |
| Pityriasis versicolor | 10 (6) |
| Folliculitis | 8 (5) |
| Onychomycosis | 6 (4) |
| Tinea corporis | 5 (3) |
| Herpes simplex | 3 (2) |
| Herpes zoster | 3 (2) |
Aesthetic lesions
Of LTRs (crude cumulative incidence) 57.1% showed cutaneous iatrogenic complications with an incidence density of 15.6% person-year and a mean time to onset of 1.6 years. The most frequent complications were: xerosis, hypertrichosis, cutaneous fragility, atrophy, teleangiectasia, gingival hyperplasia, acne, seborrheic dermatitis, alopecia, and sebaceous hyperplasia (Table III). Multivariate analysis showed that the cyclosporine-based immunosuppressive regimen was associated with a 2.5-fold increase in the risk of developing aesthetic complications as compared to the tacrolimus-based immunosuppression regimen (OR 2.6, 95% CI 1.3–5.3). The risk of aesthetic complications was 2 times greater in patients with skin phototype II–III versus patients with skin phototype IV–V (OR 2.1, 95% CI 1–4.2).
Table III. List of aesthetic complications observed in our patient population.
| Aesthetic complications | Patients affected n (%) |
| Xerosis | 46 (29%) |
| Hypertrichosis | 30 (19%) |
| Cutaneous fragility | 23 (14%) |
| Atrophy | 23 (14%) |
| Teleangiectasia | 23 (14%) |
| Gingival hyperplasia | 14 (9%) |
| Acne | 12 (7%) |
| Seborrheic dermatitis | 8 (5%) |
| Alopecia | 7 (4%) |
| Sebaceous hyperplasia | 6 (4%) |
Pre-neoplastic lesions
Eighteen percent of patients developed a pre-neoplastic skin complication (actinic keratosis), with an incidence density of 3.1% person-year. In patients with a pre-neoplastic skin complication, the association with neoplastic cutaneous lesions was statistically significant (p = 0.0006); a strong association was observed between the presence of pre-neoplastic lesions and the development of squamous cell carcinoma (SCC). Multivariate analysis showed that the development of pre-neoplastic lesions was associated with older age at transplantation (OR 1.1, 95% CI 1.01–1.12), cyclosporine-based immunosuppressive regimen (OR 2.3, 95% CI 1–5.5) and skin phototype II–III (OR 3.2, 95% CI 1.3–8.0).
Cutaneous malignancies
The percentage of patients who developed a neoplastic lesion was 8.7%, with an incidence density of 1.4% person-year. We observed a total of 14 patients, 12 males and 2 females, with skin malignancies; 10 patients (6.2%) had a single tumour, 3 patients (1.9%) had 2 simultaneous tumours and 1 patient (0.6%) had 3 simultaneous tumours. Cutaneous malignancies observed were as follows: 6 patients (31.6%) of SCC, 6 patients (31.6%) of basal cell carcinoma (BCC), 3 patients (15.8%) with Kaposi’s sarcoma, 3 patients (15.8%) with Bowen’s disease and 1 patient (5.2%) with malignant melanoma. The mean age was 52.8 ± 11 years in patients with cancer, and 46.9 ± 10.8 years in patients without cancer (p = 0.05). Malignancies were more often observed in male patients as compared to female patients (87.5% and 14.3%, respectively). The indication for liver transplant which was more frequently associated with the development of cutaneous malignancies was HCV-related cirrhosis (p < 0.05). Skin phototype was statistically related to the development of cutaneous malignancies, with a higher incidence in patients with phototype II–III (11/85, 12.9%) as compared to patients with phototype IV–V (3/76, 3.9%) (p = 0.04). No correlation was found between the emergence of neoplasms and occupational or recreational sun exposure in this group of patients. None of patients with a family history of cutaneous neoplasm developed a skin tumour, whereas 35.7% of patients with a family history of non-cutaneous cancers developed a skin tumour. Smoking or alcohol consumption was not associated with the development of cutaneous neoplastic complications.
Skin tumours were more frequently detected in patients with a cyclosporine-based immunosuppressive regimen, both as monotherapy and in association with azathioprine or mycophenolate mofetil. Of all patients who developed cutaneous malignancies, 71.4% were taking cyclosporine (p = 0.04). The role of cyclosporine in the development of cutaneous malignancies was confirmed when the group on cyclosporine therapy was compared against the group on tacrolimus therapy (p = 0.01); patients who switched from cyclosporine to tacrolimus during the follow-up period were excluded from this analysis. The second immunosuppressant (azathioprine or mycophenolate mofetil) did not show statistical correlation with the development of cutaneous cancer.
A statistically significant correlation was found between the presence of pre-neoplastic lesions and the subsequent development of neoplastic lesions: 27.7% of patients affected by actinic keratosis developed a skin tumour, whereas only 4.5% of patients without pre-neoplastic lesions presented skin cancer. Multivariate analysis demonstrated that older age at transplantation favoured the development of cutaneous malignancies (OR 1.0, 95% CI 1.0–1.2) and patients with skin phototype II–III had a 4 times higher risk to develop a neoplastic skin complication (OR 4, 95% CI 1–16.4) as compared to patients with phototype IV–V. LTRs developed a cutaneous neoplasm within ten years from the transplant, within a time of 5.7 years.
SCC and BCC were observed with the same frequency. The incidence of SCC and BCC was 0.6% person-year, with mean interval between transplantation and development of SCC and BCC of 8.9 years and 3.4 years, respectively. The development of SCC was statistically related with older age at transplantation (p=0.0002). SCC-affected patients had a mean age at transplantation of 56.1 ± 3.4 years whereas SCC-unaffected patients had a mean age of 47.0 ± 11.0. Multivariate analysis confirmed that the risk of developing SCCs was statistically related to age (OR:1.2; 95% CI 1–1.4). SCC was diagnosed only in male patients (100%). Its incidence was higher in patients with skin phototype II–III (83.3%) as compared to patients with phototype IV–V (16.7%), in smokers (83.3 %) versus non-smokers (16.7%), in patients with occupational sun exposure (66.7%) versus non-exposed (33.3%), and in patients consuming several alcoholic beverages (83.3%) versus patients consuming only wine (16.7%), or non alcohol consuming patients (0%).
A statistically significant correlation was found between SCC development and the presence of pre-neoplastic lesions (p = 0.0007): 17.9% of patients with actinic keratoses developed a SCC, whereas this complication was found in only 0.7% of patients without actinic keratoses. SCC was observed in 10% of patients bearing viral warts and only in 2.3% of LTRs without this infectious complication (p = 0.07).
The presence of BCC was statistically related to older age at transplantation (p = 0.03), with a mean age of 57 ± 5.4 years versus 47.0 ± 11.0 years in BCC-unaffected patients. Multivariate analysis confirmed that the risk of developing BCC was correlated to age (OR 1.2, 95% CI 1–1.4). BCC was more frequent in males (66.7%) and in patients with skin phototype II–III (83.3%); a borderline statistically significant association was found between BCC and sun exposure (p = 0.05). BCC was observed in 10.3% of patients with pre-neoplastic lesions and only in 2.3% of LTRs without pre-neoplastic lesions (p = 0.07).
DISCUSSION
In this study, cyclosporine-based immunosuppressive regimen, older age at transplantation and skin phototype II–III emerged as the main risk factors for developing a cutaneous complication in LTRs.
The negative impact of cyclosporine on the development of dermatological lesions was probably due to both its direct action and its effect on the immune system. The direct effect of cyclosporine was mainly responsible of the aesthetic complications, whereas infectious, pre-neoplastic and neoplastic complications were related to the immunosuppression determined by this agent.
Among the infectious complications, viral warts were frequently observed in patients undergoing a cyclosporine-based immunosuppressive regimen. It has been suggested that a high incidence of viral warts in the immunosuppressed population could be a co-factor for both pre-neoplastic and neoplastic cutaneous disease development, particularly SCC. (3). It is plausible that immunosuppressed patients may be more easily infected by oncogenic HPV, but it is also possible that development of viral warts may be a clinical sign of an over-immunosuppression, and consequently a higher risk of developing both preneoplastic and neoplastic complications.
In our investigation, 18% of patients showed pre-neoplastic complications and all of them were actinic keratoses, which are well-known precursor of SCC. The risk of developing these lesions was higher in older patients, and correlated with the use of cyclosporine and the presence of skin phototype II–III. We could not establish a statistically significant association between pre-neoplastic lesions and sun exposure, probably due to both the heterogeneity of our patient population and the difficulty to determine the amount of sunlight exposure in every patient; however, it is plausible that correlation between skin complications and older age at transplantation could be directly linked with higher cumulative absorbed doses of UV in older patients. In our patients, we observed a lower rate of cutaneous malignancies (8.7%), as compared to heart and kidney transplant recipients, in whom the incidence is more than 20% (9). The development of skin cancer was statistically related to older age at transplantation and skin phototype II–III. Univariate analysis demonstrated that the use of cyclosporine was associated with a higher risk of skin cancer, but the multivariate analysis, which included duration of immunosuppression, failed to confirm the independent role of this drug on skin tumour development. This could support the importance of the cumulative immunosuppressive load rather than the use of a specific immunosuppressant agent. Analyses considering larger number of patients may establish the true relationship between use of cyclosporine and skin cancer development.
In our study, we demonstrated a SCC/BCC ratio of 1:1, whereas in the general population the ratio is 1:4. The modification of SCC/BCC ratio is consistent with observations in heart and kidney transplant recipients, in whom the ratio is 2.2–2.4:1 (10, 11). The findings concerning SCC/BCC ratio seem to confirm the different interaction of these two cutaneous neoplasms with the immune system: SCC develops opportunistically in the immunosuppressed population, whereas BCC may develop regardless of the immunological status, due to its minor immunogenicity (11, 12).
In addition to SCC and BCC, we detected 3 cases of Kaposi’s sarcoma (KS). The incidence of KS in our patient population (1.86%) was higher compared to both the general population (2–3/1000) and LTRs investigated in other studies (0.1–0.8%) (12–14). The different results may be due to the ethnic origin of our patient population, which includes many patients from South Italy, in whom there is a genetic predisposition to this neoplasm (15).
In conclusion, improvement in post-transplant survival has led to an increase in late complications. In particular, cutaneous carcinomas still remain important complications in LTRs. Therefore, a detailed anamnestic and clinical evaluation, including age at transplantation, type of immunosuppressive regimen, presence of actinic keratoses and viral warts, may determine each patient’s risk profile and may warrant personalized prevention strategies. High-risk LTRs should be subjected to a strict follow-up protocol (dermatological evaluation every 3 months), and all other LTRs should undergo a complete skin examination at least once a year. Moreover, patients should be educated to avoid prolonged sun exposure, especially patients with skin phototype II–III. Finally, the use of tacrolimus instead of cyclosporine as the primary immunosuppressive agent may limit the development of cutaneous complications, although further studies are needed to establish if it is the cumulative immunosuppression or the use of specific agents that determines the higher risk.
REFERENCES