Kumi Aoyama1, Hiroo Amano1, Yuki Takaoka2, Ryuta Nishikomori2 and Osamu Ishikawa1
1Department of Dermatology, Gunma University Graduate School of Medicine, Maebashi, Gunma, and 2Department of Pediatrics, Kyoto University Graduate School of Medicine, Kyoto, Japan
Cryopyrin-associated periodic syndrome is an autoinflammatory syndrome caused by mutations of the CIAS1 gene (currently named NLRP3), and is characterized by periodic attacks of an urticaria-like rash, fever, headache, conjunctivitis and arthralgia. We report here a case of a 1-year-old boy with cryopyrin-associated periodic syndrome, which manifested as a recurrent skin rash in the postnatal period. Genetic analysis revealed a missense mutation of the CIAS1 gene in the mother and infant. Key words: cryopyrin-associated periodic syndrome; urticaria-like rash, NLRP3.
(Accepted November 14, 2011.)
Acta Derm Venereol 2012; 92: XX–XX
Kumi Aoyama, Department of Dermatology, Gunma University Graduate School of Medicine, 3-39-22 Showa-machi, Maebashi, Gunma 371-8511, Japan. E-mail: kumako@ac.auone-net.jp
Cryopyrin-associated periodic syndrome (CAPS) is an autoinflammatory syndrome caused by mutations in NLRP3 encoding cryopyrin (1). Three clinical types exist: familial cold autoinflammatory syndrome (FCAS), Muckle-Wells syndrome (MWS) and chronic infantile neurological, cutaneous and articular (CINCA) syndrome (1–4). FCAS is an autosomal dominant inflammatory disease and the least severe phenotype characterized by recurrent episodes of skin rash, fever, arthralgia and conjunctivitis after generalized exposure to cold (2). MWS is characterized by progressive sensorineural deafness as well as recurrent episodes of skin rash, fever and arthralgia (1). CINCA has the most severe phenotype with clinical features mimicking those of juvenile rheumatoid arthritis, including early onset, recurrent episodes of skin rash, fever, arthralgia, central nervous system involvement, and occasionally, a fatal outcome in the first or second decade of life (4).
We report here a case of CAPS in a Japanese male infant and review the clinical characteristics of the 19 cases of CAPS reported in Japanese patients.
CASE REPORT
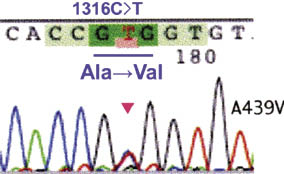
A 1-year-old boy with a skin rash was referred to our hospital in April 2010. The skin rash appeared immediately after birth, recurred intermittently, and was not relieved by antihistamines. It was unclear whether the infant had itching. The patient’s mother and maternal grandmother also had a history of a similar urticaria-like rash without itching, associated with periodic high fever of unknown origin and arthralgia. On physical examination, urticaria-like plaques 10–20 mm in diameter surrounded by erythema were distributed across the cheeks and upper and lower extremities (Fig. 1). Audiography was normal and no swollen joints were seen. Haematological examination revealed a red blood cell count of 5.53 × 106/μl and a platelet count of 415 × 103/μl, with the white blood cell count (7,900/μl) and C-reactive protein (0.02 mg/dl) within normal limits. Levels of serum amyloid A (SAA), interleukin (IL)-1β and IL-6 were not elevated and autoantibodies including antinuclear antibodies, anti-SS-A, anti-SS-B and rheumatoid factor were negative. Although the parents did not consent to a skin biopsy for histopathological examination, they did consent to investigation of NLRP3 mutation analysis using blood samples taken from the patient and his mother. A heterozygous nucleotide transition C1316T (cytosine-to-thymine transition at position 1316) was detected in exon 3 of NLRP3, resulting in a novel A439V (substitution of alanine by valine at position 439) amino acid replacement in the NOD domain (Fig. 2). The mother also had the same mutation. In light of the gene mutation analysis findings, together with the clinical features, we made the diagnosis of FCAS.
Fig. 1. Clinical appearance of the urticaria-like rash on the cheek and upper arm.
Fig. 2. Chromatograms of the NLRP3 gene at position 1316, obtained from NLRP3 gene analysis of the patient. The arrowhead indicates position 1316 on the patient's chromatogram.
DISCUSSION
Systemic autoinflammatory diseases, a recently established disease concept, are characterized by recurrent episodes of inflammation in the absence of infectious and autoimmune causes. This category includes the hereditary periodic fever syndromes, namely, familial Mediterranean fever (FMF), tumour necrosis factor receptor-associated periodic fever syndrome (TRAPS), hyperimmunoglobulinaemia D with periodic fever syndrome and cryopyrinopathies (CAPS). Moreover, other classifications have been proposed that include diseases such as Blau syndrome, Behçet’s disease and Crohn’s disease (5–8).
CAPS is caused by a mutation in the CIAS1/NLRP3 gene. NLRP3 plays a critical role in innate immunity, as it responds to intracellular pathogens and some hazardous signals. NLRP3 participates in the formation of the inflammasome, a multiprotein complex including an NLR (a Nod-like receptor) protein and an adaptor protein called apoptosis-associated speck-like protein containing a caspase recruitment and activating domain (ASC). The ASC binds and activates procaspase-1 (9, 10). Activation of the inflammasome results in conversion of pro-caspase-1 into the active protease, caspase-1, leading to caspase-1-mediated cleavage of its target molecules, such as pro-IL-1β and pro-IL-18, into biologically active forms. These cytokines participate in systemic and local responses to infection or injury (9–14). Although these cytokines can induce an urticaria-like rash, patients usually do not experience itching as there is no histamine release (15).
We reviewed 19 cases of Japanese patients with a diagnosis of CAPS (16–29). The clinical symptoms and laboratory findings are summarized in Table I. Eleven patients were male and 8 patients were female, in which 6 patients had FCAS, 4 had MWS and 9 had CINCA. Symptoms of CAPS first appeared during early childhood (0–3 years old), with skin rash being the most frequent initial symptom (n = 12). Regardless of the nature of the initial symptom, all patients developed the characteristic, recurrent urticaria-like rash, with the second most common symptom being periodic high fever (n=14), followed by arthralgia and arthritis (n = 13). Other clinical features included ocular involvement (optic nerve atrophy, chorioretinitis, uveitis (conjunctivitis)) in 12 patients, elevated levels of serum SAA in 4 patients, and deafness in 7 patients. A family history of recurrent autoinflammatory syndrome was identified in 6 cases, although it was noted that a family history was not described in 4 cases. With regard to genetic analysis, NLRP3 mutations were detected in 9 of 10 patients investigated, with one patient exhibiting NLRP3 somatic mosaicism. Somatic mosaicism of NLRP3 may result in a relatively mild phenotype of CINCA compared with common NLRP3 mutations, attributable to the difference in genotype expression among different somatic cells, namely, fewer cells in the central nervous system express the active mutation compared with those in skin (21).
Table I. Clinical symptoms and laboratory findings in 19 Japanese patients with cryopyrin-associated periodic syndrome
| Author, year (Ref.) | Disease | Age/sex | Age at onset | Symptom of onset | Family history | Gene analysis | Fever | Joint involvement | Eye involvement | Amyloidosis | Deafness | Chronic meningitis |
| Tamaki et al. 1976 (16) | MWS | 35 years/M | 3 years | Urticarial rash | + | ND | + | + | + | ND | + | – |
| MWS | 1 year/F | 3 months | Urticarial rash | + | ND | ND | ND | + | ND | – | ND |
| FCAS | 31 years/F | 2 years | Skin rash | + | ND | + | + | + | ND | ND | ND |
| Yamashita et al. 1987 (17) | FCAS | 3 years/M | 2 months | Skin rash | + | ND | + | – | + | ND | ND | ND |
| CINCA | 14 years/M | At birth | Skin rash | ND | ND | + | + | ND | ND | ND | + |
| Inamo et al. 1994 (18) | CINCA | 15 years/M | At birth | Fever, lymph node enlargement | ND | ND | + | + | + | ND | + | ND |
| Miura et al. 1997 (19) | CINCA | 0 months/F | At birth | Abdominal distension, bilious vomiting | – | ND | + | + | + | ND | ND | ND |
| Mori et al. 2002 (20) | CINCA | 7 years/M | 2 weeks | Fever | ND | ND | + | + | ND | ND | + | + |
| Saito et al. 2005 (21) | CINCA | 15 years/M | 1 year | Arthritis of the knee | – | S196N, Y570C | ND | + | + | ND | + | + |
| Gotoh et al. 2006 (22) | CINCA | 1 year/F | At birth | CRP(+), skin rash | – | + | + | – | + | ND | – | + |
| Matsubara et al. 2006 (23) | CINCA | 10 months/M | At birth | Fever, skin rash | ND | G307V | + | + | ND | + | + | – |
| Koike et al. 2007 (24) | MWS | 23 years/F | Childhood | Fever, conjunctivitis, urticarial rash | – | H312P | + | + | + | + | + | ND |
| Fujisawa et al. 2007 (25) | MWS | 12 years/M | 3rd days | Urticarial rash | + | R260W | ND | – | ND | + | ND | + |
| Kawashima et al. 2007 (26) | CINCA | 11 years/M | At birth | Fever | ND | – | + | + | – | ND | + | + |
| Itazawa et al. 2008 (27) | FCAS | 14 years/F | 4 month | Urticarial rash | + | R260W | + | + | + | + | ND | ND |
| Miyamae et al. 2010 (28) | CINCA | 10 months/F | 10 month | Fever, growth disorder | – | – | + | + | ND | ND | ND | – |
| Yamauchi et al. 2010 (29) | FCAS | 34 years/M | Infancy | Skin rash | + | Y563N | ND | ND | + | – | – | – |
| Our case | FCAS | 1 month/M | At birth | Urticaria-like rash | + | A439V | – | – | – | – | – | – |
| His mother | FCAS | 34 years/F | At birth | Urticaria-like rash | + | A439V | + | + | + | – | – | – |
MWS: Muckle-Wells syndrome; CINCA: chronic infantile neurological, cutaneous, articular syndrome; FCAS: familial cold autoinflammatory syndrome; CRP: C-reactive protein; ND: not described.
An urticaria-like rash is a typical feature of CAPS, which may be encountered by dermatologists and paediatricians, and has a high risk of frequent misdiagnosis. When infants or toddlers present with an urticaria-like rash, practitioners should recall CAPS as a differential diagnosis and examine the recurrent bouts of unprovoked inflammation in various organs other than the skin.
ACKNOWLEDGEMENT
We thank Dr Naotomo Kambe (Chiba University) for helpful suggestions.
The authors declare no conflicts of interest.
REFERENCES