Dániel Töröcsik1, Lajos Gergely2, Imre Veres1, Éva Remenyik1 and Ágnes Bégány1†
1Department of Dermatology, 23rd Department of Internal Medicine, Medical and Health Science Center, University of Debrecen, Nagyerdei krt. 98., HU-4032 Debrecen, Hungary. E-mail: dtorocsik@gmail.com
Accepted December 6, 2011.
Cryptococcosis is an opportunistic yeast infection that is the most common systemic fungal infection in immunocompromised patients. Skin involvement is a feature in 10–20% of cases of disseminated cryptococcal infection (1). We report here a case of a 63-year-old woman with Sézary syndrome (T4, N3, M0, B1) with an ulcerated preauricular tumour that developed during photopheresis with a combination of methotrexate and steroid treatment. We highlight the importance of differential diagnosis of cryptococcosis in the case of any atypical or non-healing lesions observed in an immunosuppressed patient.
Case report
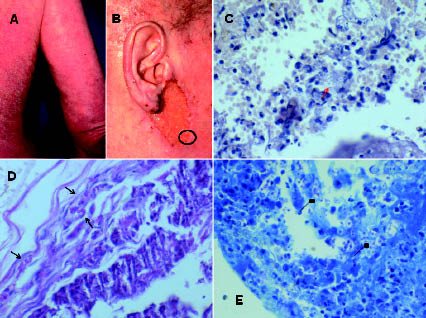
A 63-year-old Caucasian woman who had breast cancer and underwent mastectomy in 1989 followed by chemotherapy was diagnosed in 1998 with parapsoriasis through clinical signs and histological examination in the County Hospital. In 2001 she presented with generalized pruritus and erythroderma at our clinic. She responded poorly to oral psoralen and ultraviolet A (PUVA) therapy. In 2002 clinical signs (weakness, general condition, intermittent fever) were suspicious for Sézary syndrome or Cutaneous T-cell lymphoma. Sézary syndrome was confirmed in 2003 by peripheral blood examination (28% CD4+, CD7– cells), and electron-microscopy of the lymph nodes from two biopsies. At that time skin biopsies showed mild acanthosis, parakeratosis and some perivascular mononuclear cell infiltrate in the papillary dermis, whereas bone marrow biopsies were normal. After ineffective treatment with local steroid and bath PUVA she received systemic steroid plus azathioprine treatment (1 mg/kg) with moderate effect. The CD4+ cell percentage increased to 84%, consisting of 69% CD4+/CD7– cells. Due to the systemic appearance of the disease (Ann Arbor stage IV) in April 2004 one cycle of cyclophosphamide + vincristine + prednisolone (CVP) therapy was given in the Department of Internal Medicine, with poor response. She was treated with oral steroid with moderate effect. At this point another lymph node biopsy was performed that confirmed Sézary syndrome, and further treatment included total body electron irradiation in 2005 at the Oncology Center in Budapest. From February to September 2007 photopheresis in combination with methotrexate and steroid treatment had no effect on her symptoms and the skin infiltration increased, therefore methylprednisone, 8–16 mg daily, was administered constantly to control the symptoms (Fig. 1A). In May 2007, she developed a small hyperaemic nodule in the preauricular region, suspicious for basal cell carcinoma. We planned to perform a biopsy from the lesion, but the patient did not agree to the procedure at that time because of its localization. By August, at the next check-up, the lesion had a size of 2 × 3 cm with minor ulceration, and increased continuously in size to 5 × 7 cm by October (Fig. 1B). Differential diagnosis was performed for basal cell carcinoma, atypical mycobacteriosis, deep fungal infection, pyoderma, exulcerated lymphoma, spinocellular carcinoma, pyoderma gangrenosum, leishmaniasis, insect bite, burn injury, trauma, and artefact. Biopsy specimens revealed necrotic epidermis, ulceration, a granulomatous infiltrate in the dermis, and numerous round organisms with capsules measuring 2 ± 10 μm in diameter present both extracellularly and within the vacuolated spaces of macrophages (Fig. 1C). The organisms were also stained with Giemsa and showed periodic acid-Schiff (PAS)-positive reaction (Fig. 1D and E). Serology for Cryptococcus antigen was positive in the blood. Chest X-ray and computed tomography (CT) revealed Cryptococcus infection of the lung, cerebrospinal fluid was negative for the presence of Cryptococcus and there were no signs or symptoms of meningeal involvement.
Fig. 1. (A) Generalized exfoliative erythroderma of the patient with advanced Sézary syndrome before extending photopheresis treatment with a combination of methotrexate and steroid. (B) Ulcer affecting the pre-auricular region mimicking basal cell carcinoma that developed during immunosuppressive treatment. Note the biopsy site (circle). (C) Histological examination of the skin biopsy from the ulcer showed innumerable thick capsulated round organisms measuring 2 ± 10 μm both extracellularly and within the vacuolated spaces of macrophages (red arrows) (haematoxylin and eosin; original magnification × 40). (D) Cryptococcal organisms stain red with periodic acid-Schiff (PAS) (black arrows) (original magnification × 100) and (E) blue with Giemsa stain (diamond arrows) (original magnification × 40).
In October 2007 the patient started receiving intravenous amphotericin B and fluconazole. Despite all our efforts Cryptococcus antigenaemia was still detected. The patient died 6 weeks later from acute cardiac and renal failure. Autopsy revealed cutaneous cryptococcal infection in the skin of the submammal region of the thorax and in the lungs.
Discussion
Cryptococcal species are yeast-like fungi. Based on their virulence they are classified as pathogenic or non-pathogenic. Classically, C. neoformans is the only pathogenic cryptococcal species present in high concentrations in pigeon faeces, but also in soil, fruit, and other sources in nature, such as eucalypt reservoirs. It includes four distinguishable serotypes: A (C. neoformans var. grubii) has a worldwide distribution; D (C. neoformans var. neoformans) found mostly in Europe; and B and C (C. neoformans var. gattii), which are limited to tropical and subtropical areas (2, 3).
Cryptococcus infection is acquired by inhalation and resides in the lung, mostly in the immunocompromised host, as was the case in our patient, due to Sezary syndrome and continuous steroid immunosuppressive treatment with photopheresis extended with a combination of methotrexate. Infection can also involve patients with intact immune systems who are predominantly infected with C. neoformans var. gattii (4). The infection can resolve or disseminate, mostly spreading to the meninges, but bones, viscera and the skin can also be involved. In the diagnoses of Cryptococcus infection, culture from smears of body fluids, secretions, exudates, or other specimens is definitive, but X-ray and serological examination are also of importance.
Involvement of the skin can result in a great variety of lesions, most commonly affecting the face and neck, from papules, nodules, acneiform lesions, granulomas, herpetiform vesicles, abscesses, and ulcers, resembling other cutaneous disease, such as molluscum contagiosum, vasculitis, Kaposi’s sarcoma, varicella, basal cell carcinoma, cellulitis, cutaneous ulceration, atypical mycobacteriosis and whitlow (5–8). The two forms of histological manifestation are gelatinous and granulomatous reactions. While the granulomatous type results in pronounced tissue reaction, with histiocytes, giant cells, lymphocytes, and fibroblasts, with a low number of yeasts, that vary in size from 2 to 20 μm, in the gelatinous type, masses of organisms occur, with the accumulation of cryptococcal capsular polysaccharide causing mucoid degeneration of the invaded tissue, with only minimal signs of inflammation (6).
Treatment of the systemic infection includes appropriate antifungal drugs, in which the mainstay is intravenous amphotericin B in combination with flucytosine, which is often followed by fluconazole for many months or, depending on the patient’s immune status, even life-long. If fluconazole is not available or is contraindicated, acceptable alternatives include itraconazole, or extended-spectrum azoles (voriconazole and posaconazole). Occasionally, localized cryptococcal infections of the lung not responding to medical therapy may require surgical resection for cure (9). In the case of cutaneous Cryptococcus infection successful treatment with oral fluconazole alone has also been reported, and incision, with local irrigation and debridement, topical application of anti-inflammatory agents and antifungal agents was also recommended (8, 10).
Our case illustrates the importance of serological tests with histological examination, and pathogen-culturing from any atypical or non-healing lesions observed in immunocompromised patients for an accurate diagnosis of opportunistic infection. Importantly, a primary infection of the lung and disseminated infection involving the central nervous system may be present with dermatological rather than pulmonary or neurological manifestations (11).
The authors declare no conflicts of interest.
The authors pay tribute to Dr Agnes Begany, the outstanding dermatologist and person, who stays with us in our thoughts and words.
References