Andrea Bassi1, Meena Arunachalam1, Vincenza Maio2 and Elisa Difonzo1
1Department of Critical Care Medicine and Surgery, Division of Dermatology, and 2Division of Pathological Anatomy, University of Florence, Piazza dell’Indipendenza, 11, IT-50129 Florence, Italy. E-mail: bassi76@interfree.it
Accepted February 23, 2012.
Diffuse dermal angiomatosis (DDA) is a type of reactive skin angioproliferation. Clinically, this rare disorder presents as red-violet purpuric papules and/or plaques (some with a greater tendency towards necrosis and ulceration), which can be localized in any body area, but is most often seen in the upper and lower extremities. Histological examination is fundamental for the diagnosis, and is characterized by varied patterns of lobular or diffuse hyperplasia of endothelial cells at the extravascular level. We describe here a case of DDA in a 42-year-old man with an arterio-venous fistula and Wegener’s granulomatosis.
CASE REPORT
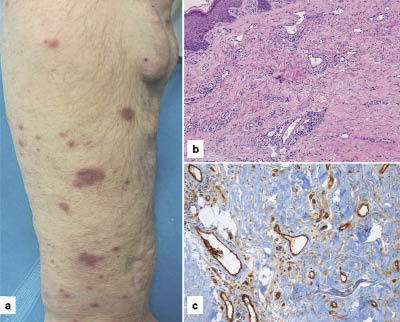
A 42-year-old man presented to our clinic due to a 2-year history of non-painful, hard, reddish-purple plaques and nodules on the right arm nearby a haemodialysis-related arterio-venous fistula (Fig. 1a). During this time period, the lesions had increased slightly in number and volume without signs of regression. Ten years previously, the patient had pulmonary and renal manifestations compatible with Wegener’s granulomatosis. This clinical diagnosis was confirmed upon biopsy of both the lungs and the kidneys, which showed granulomas and vasculitis. He was treated with mycophenolate mofetil, methylprednisolone, and ticlopidine prior to our observation. Cutaneous signs of Wegener’s granulomatosis, such as necrotizing, granulomatous vasculitis, were not visible at clinical presentation. Complete blood count with differential and a complete metabolic panel denoted high fibrinogen, creatinine, C-reactive protein, anti-neutrophil cytoplasmic antibody, white blood cell, and neutrophil levels, and a low haemoglobin level. Prothrombin, activated partial prothromboplatin time, and D-dimer levels were unremarkable. Histological examination performed on a purpuric lesion showed diffuse capillary proliferation in the superficial and deep dermis (Fig.1b). A few vascular structures were dilated by erythrocytes and contained a prominent endothelium. Immunohistochemistry showed positive CD31 staining, confirming the presence of endothelial cells in the dermal infiltrate (Fig.1c) and negativity for HHV-8.
Fig. 1. (a) Reddish-purple plaques and nodules localized on the right arm close to an arterio-venous fistula. (b) Histopathological examination shows a diffuse proliferation of capillary vascular structures in the superficial and deep dermis (haematoxylin-eosin stain; magnification × 20). (c) CD31 stains a prominent endothelium decorating the vascular structures of variable size and shape in an interstitial pattern among collagen bundles (magnification × 20).
DISCUSSION
The clinical presentation of our patient suggested 3 cutaneous reactive angiomatoses, which can resemble one another and can occur in association with an arteriovenous fistula: DDA, reactive angioendotheliomatosis, or acroangiodermatitis (pseudo-Kaposi’s sarcoma). A distinction is made between them on histological examination (3, 4). Both histological and immunohistochemistry suggested DDA, a reactive, dermal, vascular lesion with a distinct pattern (3). While DDA demonstrates diffuse endothelial extravascular hyperplasia in the superficial and deep dermis between collagen bundles, reactive angioendotheliomatosis is characterized by endothelial proliferation within the lumen of dermal vessels. Pseudo-Kaposi’s sarcoma, by contrast, exhibits a slight endothelial proliferation and formation of new thick-walled vessels, often in a lobular arrangement in the papillary dermis. Kaposi’s sarcoma (HHV-8+) might also be considered in the differential diagnosis, as this condition is characterized by red-violet patches, plaques or nodules, located mainly on the extremities; its histological profile consists of spindle cells and vascular structures with a characteristic clefting pattern (vascular slits). However, intravascular proliferation, as seen in DDA, is not present in pseudo-Kaposi’s sarcoma.
According to current literature, cutaneous reactive angiomatoses, such as DDA, might be attributed to occlusive or inflammatory vasculopathic processes in the vascular tree, which result in the formation of microthrombi and subsequent hypoxia (3). Subsequently, histiocytes are recruited and hyperplasia of endothelial cells and pericytes occurs. The former plays a role in the reabsorption of microthrombi. We hypothesize that both arteriovenous fistula and the patient’s concomitant Wegener’s granulomatosis resulted in ischaemia. This phenomenon induces vascular endothelial growth factor (VEGF), which in turn stimulates endothelial extravascular hyperplasia, as seen in DDA (3).
While no definitive therapeutic protocols exist for cutaneous reactive angiomatoses, systemic or topical corticosteroids are used for their anti-angiogenetic properties. The results are not always effective (1, 3). Use of systemic corticosteroids for an underlying Wegener’s granulomatosis did not prevent a progressive diffusion of DDA over the entire forearm of our patient. The topical corticosteroid, 0.1% methylprednisolone aceponate, was utilized in our patient without improvement at a 1-year follow-up. It is possible, however, that these lesions spontaneously improve or disappear.
DDA is a very rare manifestation, according to the current literature, which can appear secondary to an arteriovenous fistula in patients with chronic renal insufficiency who undergo haemodialysis. To our knowledge, the present case is only the third reported (1, 2). Sommer et al. (2) describe the concomitant presence of Wegener’s granulomatosis as in our patient, suggesting that DDA is favoured by systemic diseases involving occlusive or inflammatory vasculopathy.
ACKNOWLEDGEMENT
The authors thank Professor Daniela Massi, MD, for assisting with the histopathological assessment.
The authors declare no conflicts of interest.
REFERENCES