


Dimitra Kiritsi1, Arti Nanda2, Jürgen Kohlhase3, Carsten Bernhard3, Leena Bruckner-Tuderman1,4, Rudolf Happle1 and Cristina Has1*
1 Department of Dermatology, University Medical Center Freiburg, Hauptstrasse 7, DE-79104 Freiburg, Germany, 2As’ad Al-Hamad Dermatology Center, Al-Sabah Hospital, Kuwait, 3Center for Human Genetics Freiburg, and 4Freiburg Institute for Advanced Studies, University of Freiburg, Freiburg, Germany *E-mail: cristina.has@uniklinik-freiburg.de
Accepted May 21, 2013; Epub ahead of print Oct 3, 2013
Epidermolytic ichthyosis (EI, MIM#113800) is a rare genetic disorder of keratinisation with the incidence estimated to be less than 1 in 100,000. The phenotype is characterised by congenital erythroderma, blistering and erosions of the skin, which cease in the first months of life and are followed by hyperkeratosis and verrucous scaling from early childhood (1). The disorder is dominantly inherited and caused by mutations in the genes encoding keratin 1 or 10 (KRT1, KRT10) (2), which are expressed in the suprabasal epidermal layers (3). The histological findings in EI, comprise thickened epidermis, epidermolysis within the suprabasal layer, and vacuolar degeneration and presence of keratinocyte granules in the granular layer (4). In addition to the generalised form of EI, epidermolytic naevi following the Blaschko’s lines, representing segmental mosaicism for KRT1 or KRT10 mutations have been described in a few patients. Mutations in KRT1 (5) and KRT10 (1, 6, 7) were found in the lesional but not in non-lesional skin, and in some (6), but not all cases (1, 5), the respective mutation was found at low allelic levels in DNA from lymphocytes. If the germ line is also affected, patients with epidermolytic naevi are at risk of transmitting EI to the offspring.
Case report
Here, we report on a 5-year-old boy with widespread hyperkeratotic, verrucous plaques being more pronounced in the folds, but affecting almost the entire body surface (Fig. 1). On this background, sharply limited normal-appearing areas were present next to severely verrucous skin in a band-like or patchy arrangement on the limbs and trunk (Fig. 1A–C). Palms and soles showed minimal focal keratoses. To address the molecular background of this extensive EI with patches of normal appearing skin, EDTA blood was obtained, as well as skin biopsies from an unaffected patch on the right flank (biopsy 1, Fig. 1A), a severely verrucous area next to it (biopsy 2, Fig. 1A), and a hyperkeratotic area on the chest (biopsy 3, Fig. 1B). Haematoxylin and eosin staining of the affected skin samples was consistent with epidermolytic hyperkeratosis, whereas the clinically healthy skin patch showed normal morphological features (Fig. 1D). Keratin 1 was strongly reduced in affected skin, but stained comparably to the control in unaffected skin (Fig. 1E). Keratin 10 staining revealed a perturbed filamentous cytoskeleton with aggregation of tonofilaments around the nucleus (Fig. 1F). Surprisingly, no KRT1 or KRT10 mutation was detected, suggesting that the disorder was due to a de novo postzygotic mutation mainly present in the affected skin. Therefore the analysis was extended to DNA from the skin of the patient. In both keratinocytes and fibroblasts from the affected skin the mutation c.1349G>C; p.Arg450Pro in exon 6 of KRT10 was disclosed in a heterozygous state. To the best of our knowledge, this allelic variant has not been reported before (Human Gene Database; HGMD Professional 2012.4). It is predicted to be disease-causing Polyphen 2 and it is not referenced as a SNP. This variant is located in the helix 2B domain of KRT10, in close vicinity to amino acids which are known to be mutated in patients with EI (Gln447Pro, Tyr449Asp, Tyr449Cys, Leu452Pro) and two residues N-terminally of the highly conserved LLEGEG sequence (amino acids 452–457) (1). When re-examined, the DNA sequence derived from lymphocyte DNA of the patient demonstrated the mutant allele at a low level, of about 10%, which had been considered as background in the initial analysis (Fig. S1; available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1695). The same result was obtained with DNA extracted from keratinocytes and fibroblasts isolated from the normal-appearing skin (Sample 1, Fig. 1G). The mutation was absent in the DNA of both unaffected parents (Fig. S1). These findings confirmed that the patient had an epidermolytic naevus involving about 80% of the integument. Based on the presence of the mutation in keratinocytes, fibroblasts and lymphocytes, we speculate that it occurred very early during embryonic development. Since these tissues are derived from both ectoderm and mesoderm the time point was probably before the 4-cell stage (9). The extensive involvement of the skin suggested that mutant keratinocytes possess a selection advantage. To address this, we analysed epidermal proliferation, which clearly demonstrated significantly increased Ki-67-positive keratinocytes in areas with epidermolytic hyperkeratosis (Fig. 1H), probably as a response of the basal keratinocytes to the defective cytoskeleton caused by the KRT10 mutation (10), thus providing them with growth advantage.
Because of the proximity of the normal-appearing areas to markedly verrucous lesions (Fig. 1A) we investigated whether these result from a recombination event causing loss of heterozygosity (11), and leading to a “twin spot phenomenon” (12), as described in Darier’s disease and neurofibromatosis (13). Laser dissection microscopy was employed to isolate keratinocytes from a severely affected area, however no evidence for homozygosity of the mutation was found.
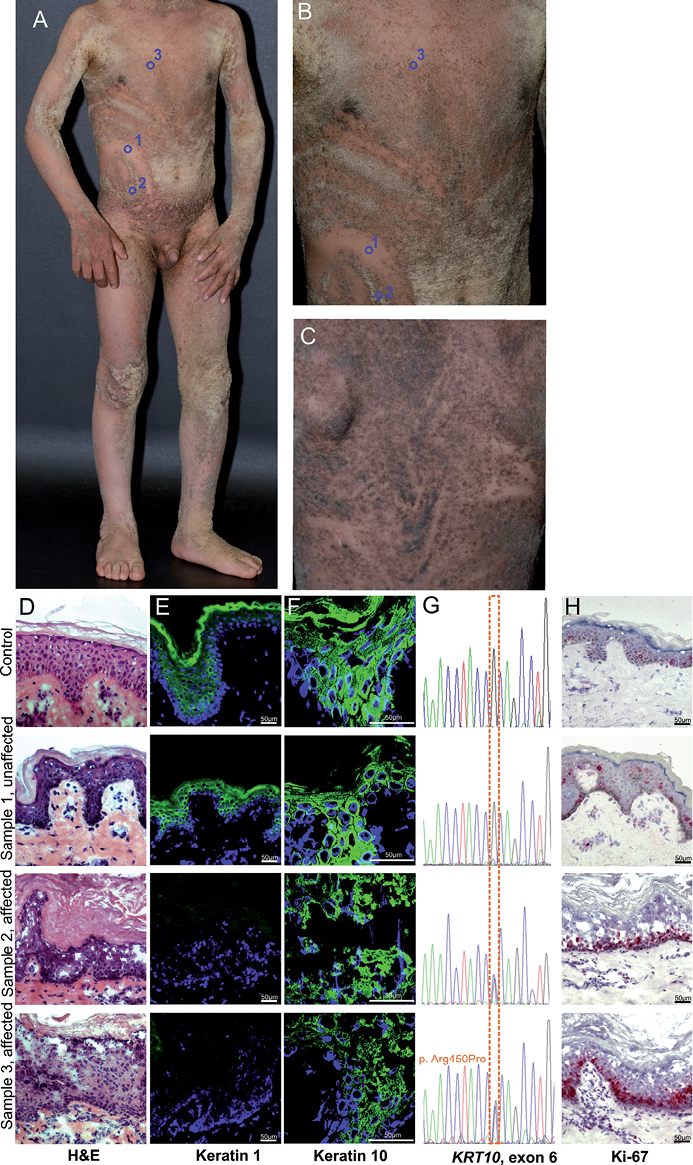
Fig. 1. Clinical features suggestive of epidermolytic ichthyosis in the 5-year-old patient, morphological analysis of his skin and identification of the disease-causing mutation. (A–C) Linear or patchy areas of normal-appearing skin, following the Blaschko lines on epidermolytic hyperkeratosis background are present on the flank (A) and back (B) of the patient. Hyperkeratotic verrucous plaques are more pronounced in the folds, but affect almost the entire body surface. The biopsy sites are depicted by blue circles. (D) H&E staining of an unaffected patch showed unremarkable skin structure, whereas in both hyperkeratotic areas the characteristic signs of epidermolytic hyperkeratosis were present. (E) IIF staining of keratin 1 was comparable to control skin in the unaffected patch on the right flank, but strongly reduced in the hyperkeratotic area of the chest and in the severely hyperkeratotic, verrucous skin of the right flank. (F) IIF staining of keratin 10 revealed aggregation of the tonofilaments around the nucleus. (G) Partial sequence of KRT10 exon 6 showed the heterozygous mutation p.Arg450Pro in less than 10% of the allelic levels in DNA derived from the unaffected skin sample 1, whereas in DNA isolated from both affected samples (2, 3) it represented around 50% of the allelic levels. (H) Ki-67 staining was strongly increased in samples 2 and 3 derived from affected skin and comparable to the normal skin in the unaffected sample 1. Indirect immunofluorescence (IIF).
Methods: IIF staining for keratin 1 (clone 34ßB4, Enzo life Sciences, Lörrach, Germany) and 10 (LH2, Santa Cruz, Heidelberg, Germany) was performed as described before (8). Epidermal proliferation was evaluated using immunohistochemical staining with antibodies to Ki-67 (8). Mutation analysis of the KRT1 and KRT10 genes were analysed as described (9, 10) in DNA extracted from EDTA blood of the patient, following written informed consent, in adherence to the Declaration of Helsinki principles. Keratinocytes and fibroblasts cultured as described before (8) were used for DNA extraction with the QIAamp DNA FFPE Tissue Kit (Qiagen, Hilden, Germany). Laser dissection microscopy was employed to isolate keratinocytes from a severely affected area, which were subjected to DNA isolation, nested PCR and sequencing of the region spanning the mutation as described before (8).
DISCUSSION
The hypothesis that normal skin patches in the affected skin represented revertant mosaicism, and together with neighbouring, severely affected areas result from a “twin spot phenomenon” (12, 13), could not be confirmed on a molecular level. Nevertheless, because of the extensive skin involvement, the term epidermolytic naevus is rather inappropriate in the present case, for which we propose the designation EI with postzygotic mosaicism.
In our patient, the mutation was initially missed because of the very low levels of the mutant allele in the lymphocyte DNA. The presence of the mutation in the germ line determines the risk for transmission to the offspring, rendering the identification of the disease-causing mutation highly relevant for prenatal testing. These findings have also implications for mutation analysis in patients with genetic disorders, because postzygotic mosaicism may explain cases in which mutations are not disclosed by routine screening.
ACKNOWLEDGEMENTS
We thank the patient and his family. The excellent technical support by Kaethe Thoma, Margit Schubert, Ioannis Athanasiou and Annegret Bedorf is gratefully acknowledged. This work was supported by the Network Epidermolysis bullosa grant from the Federal Ministry for Education and Research (BMBF) and the E-RARE grant “RevertantEB” to LBT., and the Excellence Initiative of the German Federal and State Governments and Freiburg Institute for Advanced Studies, School of Life Sciences to LBT, the “Theodor-Nasemann Scholarship” from Galderma Förderkreis and the DFG grant 1795/1-1 to D.K. and the DFG grant 5663/2-1 to C.H.
The authors declare no conflict of interest.
References


