


Niels Sandø1, Kristian Kofoed2, Claus Zachariae3 and Jan Fouchard1
1Disease Prevention & Local Services, Danish Health and Medical Authority, Copenhagen, 2Department of Dermato-Venereology, Copenhagen University Hospital, Bispebjerg and 3Department of Dermato-Allergology, Copenhagen University Hospital, Gentofte, Denmark
In January 2009 the human papillomavirus (HPV) vaccine was included in the Danish childhood vaccination programme for girls aged 12 years. A catch-up programme for girls up to 16 years of age was started a couple of months earlier. Based on national register data, anogenital wart (AGW) incidences between January 2001 and December 2011 were estimated. We used χ2 analysis to identify significant trends in proportions of patients diagnosed with AGW in the period before and after inclusion of the HPV vaccine in the program. The development of chlamydia infections was included in this study as a proxy for possible behaviour changes that could affect the AGW incidence. Between 2008 and 2011, a 50% (95% CI 44–56) decrease in AGW incidence was seen among 15–19-year-old men (p = 0.041), from 5.2 to 2.6/1,000. Among women, a 67% (95% CI 63–72) decrease from 11.7 to 3.8/1,000 was seen (p < 0.0001). The decline in frequency of AGW in young Danish women seems to result from the high coverage of the HPV vaccination programme and young men probably benefit from herd immunity. Key words: anogenital warts; condyloma; human papillomavirus; quadrivalent human papillomavirus vaccine; Denmark; herd-immunity.
Accepted Jun 27, 2013; Epub ahead of print Oct 17, 2013
Acta Derm Venereol
Kristian Kofoed, Department of Dermato-Venereology d41, Copenhagen University Hospital Bispebjerg, Bispebjerg Bakke 23, DK-2400 Copenhagen, Denmark. E-mail: kkofoed@hotmail.com
Anogenital warts (AGW) is caused by human papillomavirus (HPV) which is one of the most common sexually transmitted infections (STI) (1–3).
AGW is a treatable and benign condition. The treatment can, however, be a lengthy process with economic consequences for the health system (1, 2). Studies have shown that successful care for an AGW patient requires a mean of 5.7 physician visits per episode for men, and 6.3 physician visits per episode for women (2). AGW has emotional consequences for patients as well, and is reported to affect the patients’ self-esteem, their sexual relations, cause fear of relapse and long-term development consequences in terms of cervical cancer (3, 4).
About 90% of all AGW cases are caused by HPV types 6 and 11 (5, 6). In clinical trials the quadrivalent HPV vaccine (Gardasil®) has proven highly effective against infection with HPV types 6 and 11 and thus against the development of the majority of AGW among men and women (7–9).
In January 2009, free HPV vaccination of young girls born 1996 or later (given at age 12) was included in the Danish childhood vaccination programme. The primary focus was the prevention of cervical cancer, thus boys were not included in the programme. It was expected that herd immunity would develop and subsequently provide protection for the boys. A catch-up programme was introduced in October 2008 to provide free HPV vaccination for girls aged 13–15 (born in 1993–1995), which was in effect until 31 December 2010. The vaccine that was chosen was Gardasil®. An information campaign was launched to ensure high vaccination coverage. The information campaign included direct mail to all girls aged 12–15 and their parents, information materials to general practitioners, school nurses and a designated website.
Prior to the free vaccination programme, the vaccine had been available in Denmark at a cost of approximately €500 per person for 3 doses (10).
A relatively high coverage of the HPV vaccination programme was achieved immediately after the introduction of the programme and maintained in the years after. Around 80% of the girls eligible for the vaccination programme received all 3 doses of vaccine, and around 90% received the first dose.
The coverage of the HPV-vaccine for girls born in 1987–1991, who were not covered by the free vaccination programme, varies between 11 and 22% and is highest among the youngest and lowest among the oldest.
The effect of the HPV vaccination programme on the incidence of cervical cancer cannot be established in the near future, as the time from HPV (type 16 and 18) infection to the development of cervical cancer is several years or even decades (11). The median time from HPV (type 6 and 11) infection to the development of AGW is only around 3 months (12). Thus, the vaccine effect on AGW is an important indicator for the future effect on the incidence of cervical cancer, which reports from Australia and Sweden already have indicated (13, 14).
The Danish health service has a long tradition of recording health service provisions and redeemed prescriptions. This allows us to study the national incidence of AGW and the use of AGW medication before and after the introduction of the HPV vaccination programme.
MATERIAL AND Methods
Data collection
AGW is not a notifiable infection in Denmark, thus no national surveillance data exist. To assess the annual incidence of AGW, data from the Register of Medical Products Statistics were combined with data from the National Patient Register. All patients living in Denmark are included in these registers, and linkage between the registers is possible by using the personal identity numbers (CPR). The number of persons who were treated for AGW in the different age groups was assessed by calculating the total number of:
A person was considered to have a case of AGW during the calendar year if he/she appeared in one of these registries. Only one episode contribution was allowed per person per calendar year because the aim was to estimate the proportion of individuals seeking or receiving treatment for AGW during that year. The figures derived indicate the number of people who have received treatment in a given year. As there have been no changes in the treatment procedures or in the reporting system, the figure is considered suitable as a proxy indicator for AGW incidence. Patients prescribed imiquimod were not included.
Chlamydia is a notifiable infection in Denmark. The National Institute for Health Data and Disease Control (Statens Serum Institute) receives quarterly data on laboratory diagnosed chlamydia from clinical microbiology and biochemical departments. It is estimated that a substantial number of cases are not diagnosed due to factors, such as the high proportion of asymptomatic chlamydia infections. Chlamydia infections are included in this study as a proxy for possible behavioural changes that could affect the AGW incidence.
Population size: Mid-year population data from the national statistical bureau in Denmark (Statistics Denmark) has been used to assess the incidence of AGW and chlamydia in the age groups. Mid-year figures are used to minimise the effect of deaths, migration and immigration.
The entire population of young people aged 15–34 in Denmark in 2001–2011 has been included in this study. The size of the 5-year age groups 2001–2011 is presented in Table SI1.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1721
The vaccine coverage for girls, who were not included in the national vaccination programme, was assessed by identifying the number of claimed prescriptions for Gardasil, used by girls in the specific age group. The number was divided by 3, as 3 doses are needed for a complete vaccination.
Statistical analysis
The pre-vaccination period was from 2001 to 2008, and the vaccination period was from 2009 to 2011. To compensate for changes in population size during the investigated periods we calculated the incidence/100.000 persons of AGW and chlamydia and used these data in our comparisons of proportions. We used χ2 tests to identify significant trends in proportion of people with warts and in proportion of people with AGW compared with the proportion of people with chlamydia in the pre-vaccination and post-vaccination periods. Statistical analyses were done with GraphPad Prism version 5, and p < 0.05 was regarded as significant.
Results
The mid-year population size and the number of men and women aged 15–34, who have received treatment for AGW, from 2001–2011 is shown in Table SI1.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1721
Fig. 1 show the development in the number of men and women (per 1,000) treated for AGW 2001–2011, in the different age groups. All age groups have experienced a statistically significant increase between 2001 and 2008 (p < 0.0001). Subsequently, among young women aged 15–19 there was a significant decrease of 67% (95% CI 63–72; p < 0.0001). For young men in the same age group there was also a significant reduction of 50% (95% CI 44–56; p < 0.0001), between 2008 and 2011.

Fig. 1. Anogenital warts treatments per 1,000 men (A) and women (B) aged 15–34 during 2001–2011.
In men and women aged 20–24, there was a significant decrease of 6% (95% CI 5.1–7.1; p = 0.041) among men, and of 18% (95% CI 16–19; p < 0.0001) among women, between 2008 and 2011.
For men aged 25–29 there were no significant changes from 2008–2011, whereas in the same age group of women there was a statistically significant increase (p = 0.0015) of 11%. For men aged 30–34, there was a significant increase of 13% (95% CI 10–15; p = 0.0108), between 2008 and 2011. For women in this age group, there were no significant changes 2008–2011.
The incidence of chlamydia for men and women between 2001 and 2011 is shown in Fig. 2.
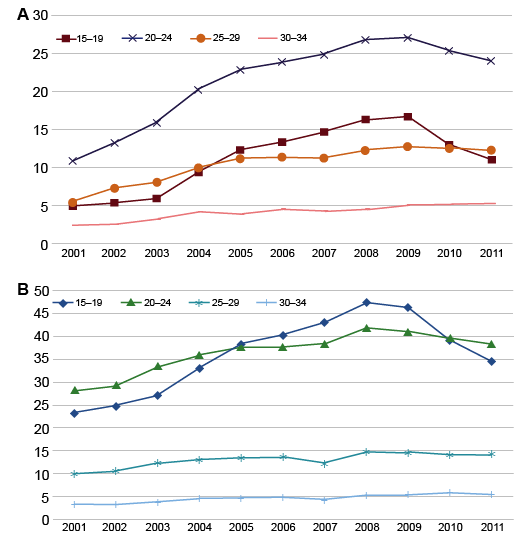
Fig. 2. Chlamydia incidence per 1,000 men (A) and women (B) aged 15–34 during 2001–2011.
For all age groups and sexes there was an increase in the incidence between 2001 and 2008. However, among girls aged 15 to 19 there was a 27% (95% CI 26–29) decrease between 2008 and 2011 (from 47.4 to 34.6/1,000). For boys aged 15–19 there was a 33% (95% CI 30–35) decrease between 2008 and 2011 (from 16.3 to 11.0/1,000). For women aged 20–24, there was an 8.6% (95% CI 7.7–9.5) reduction (from 41.9 to 38.3/1,000) 2008–2011, and for men in this age group, the decrease was 10% (95% CI 9.2–12 from 26.8 to 24.0/1,000). Among the age groups 25–34 the incidence had stagnated between 2008 and 2011.
The indexed incidence of both AGW and chlamydia among men and women aged 15–19, is shown in Fig. 3.
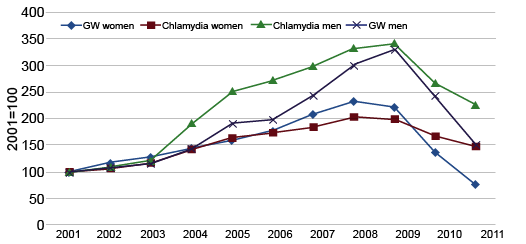
Fig. 3. Anogenital warts treatments and chlamydia in men and women aged 15–19 during 2001–2011. Index 2001 = 100.
It can be noted that the incidence in AGW and chlamydia in the age group 15–19 followed the same trends. The decrease in AGW incidence was significantly more pronounced than the decrease in chlamydia incidence (p < 0.0001), however, the increase in AGW before 2009 was also significantly more pronounced than the increase in the chlamydia incidence (p = 0.0293).
Among the young men aged 15–19, the statistical analysis did not indicate differences in the development of the conditions before 2009. From 2008 the decrease in AGW was significantly more pronounced than the decrease in the chlamydia incidence (p < 0.0001).
Among women in the group aged 20–24 years both the increase (2001–2008) and the decrease (2008–2011) of AGW were more significant than the increase and decrease in the chlamydia incidence (p < 0.0001). For men aged 20–24, the decrease in AGW was not significantly different from the decrease in the chlamydia incidence.
Discussion
Unlike other studies, this study entails national population data on AGW before and after the introduction of free HPV vaccine in the routine vaccination programme. Using chlamydia as a proxy for possible behavioural changes, the study compares the development in AGW incidence with chlamydia incidence.
The data presented showed significant decrease in the incidence of AGW among men and women aged 15–19, since the introduction of the HPV vaccination programme, and the development was independent of the development of chlamydia incidence. Similar but not as marked effects have been reported in Sweden, US, New Zealand, and Australia (13–16). However, these studies have not compared the development in AGW incidence with chlamydia. The results indicate that the HPV vaccination programme has had an independent and marked effect on AGW. Taking into account that girls aged 19 in the group of 15–19 years old were not covered by the vaccination programme in 2011, it is likely that the rapid decline in AGW will continue in the years to come.
The fact that both AGW and chlamydia increased between 2001 and 2008 may have been influenced by the following factors: From the mid 1990s to 2004, there were no national campaigns in Denmark on STIs, and only 12% of young people aged 15–19 perceived themselves to be at risk for a chlamydia infection (17). Between 2004 and 2008, the National Board of Health implemented national campaigns on chlamydia, and recommended chlamydia testing for people with risk behaviour. Between 2003 and 2008, the number of people tested for chlamydia increased by 26%, from 268,008 in 2003 to 338,150 in 2008. This could explain part of the increasing incidence, however, the positive rate also increased by 25% (from 6.9% in 2003 to 8.6% in 2008) which could indicate an actual increase in the spread of the disease, or that more people with risk behaviour had been tested (data from Statens Serum Institut, EPI-Nyt, week 20, 2009).
Moreover, when more people go to their GP to be examined for chlamydia, it is likely that more people with AGW will be found. Lastly, the increase in chlamydia incidence 2001–2004 may also have been influenced by the introduction of the more sensitive DNA tests. Thus, the recorded increase in AGW and chlamydia incidence may to an extent be a consequence of the above mentioned factors, as well as an actual increase in the incidence.
The fact that both AGW and chlamydia decreased between 2008 and 2011 may be influenced too by the following factors (in addition to the vaccine, which is examined in this paper): The national HPV vaccination campaign in 2008 linked cervical cancer with unprotected sex. This might have increased the awareness of risk associated with infection, and hence condom use. Also, young girls in the catch-up programme have been informed about safe sex when they visited the GP for the HPV vaccination. Lastly, the National Board of Health implemented national campaigns on condom use from 2009.
The decrease in AGW and chlamydia incidence 2008–2011 may have been influenced by a behavioural change in the population, thus the decrease in AGW incidence may not solely be attributable to the vaccine itself. Therefore, it has been essential to determine whether the decrease in AGW incidence is significant not only in itself, but also to assess whether it is statistically associated with the chlamydia incidence.
When focusing on young men aged 15–19, it is worth noticing that the onset of the decline in AGW incidence seems to be delayed compared to women. This is, however, to be expected as the effect of the vaccine has to be passed through young women. The data indicate the development of herd immunity among young heterosexual men. It should be noted that we have no data on sexual preference, thus we are not able to distinguish between men having sex with women (MSW) and men having sex with men (MSM). Studies have shown a higher prevalence of AGW among MSM (4, 15, 18–20) and in theory MSM should not benefit from a vaccination programme for girls. Therefore, the herd immunity could be even more significant among MSW.
The substantial decrease in AGW incidence among young people covered by the free vaccination programme follows experiences from Melbourne, Australia, where vaccine coverage of 65–70% has been achieved (13, 15, 16). The relatively high coverage of the vaccination programme in Denmark is likely to be a key point in achieving both the initial decline in the incidence among women, and in protecting young men through herd immunity.
Among young people aged 20–24, a much smaller proportion of girls has been vaccinated. The relatively low vaccine coverage in this age group could explain the less marked reduction of AGW incidence. However, there has been a statistically significant decline among both men and women in this age group, but it is only among women that the decrease in AGW is statistically independent of the development in chlamydia incidence. These results do not provide the evidence of herd immunity among men aged 20–24. These findings correlate with results from Sweden, where they have an opportunistic vaccination programme at a cost of approx. €500 for 3 doses. In Sweden, they found a 17% reduction in AGW incidence from 2006–2010, with vaccine coverage of 25–30% (14). This is equivalent with the 15% reduction among women and 18% reduction among men in this study. However, in the Swedish study no significant reduction was seen among men.
In the age group 25–34 there was no significant decrease among women, which is expected, as there is no vaccination programme for this group, and as there were only few people who had paid to be vaccinated. Among men in this age group the continued increase in AGW after 2009 for the group aged 25–29 was found to be significant, which puts the decrease, and the indications of a herd immunity among young men aged 15–19, into perspective.
Our study has some limitations. There will be a possible systematic underrepresentation of the AGW cases, as treatment with imiquimod has not been included. Imiquimod is used to treat AGW as well as other diseases such as actinic keratosis and basal cell carcinoma. Therefore, including imiquimod in the data would have caused an overrepresentation of cases. However, as treatment with Podophyllotoxin is the first-line treatment of AGW, many of the patients would be registered by their first contact. Furthermore, patients who receive their first-line treatment at gynaecologists or dermatologists and venereologists in private practice are not registered, and therefore not included in these data, unless they have received treatment with Podophyllotoxin or have been referred to a hospital or a sexual health clinic.
Moreover, the HPV-vaccination coverage among young girls, who are not covered by the free HPV-vaccination programme, can only be an indicative figure, as a number of girls will not use all 3 doses, but only one or two, and some girls from Copenhagen and surroundings might have used their prescription in Sweden, where Gardasil was cheaper. These girls were not included in the data, and finally, some GPs and gynaecologists have sold the vaccine directly, and this will not be included in the figure either.
Conclusion
This study shows a remarkable and significant relationship between the incidence of AGW among young women aged 15–19, and those covered by the HPV-vaccination programme. Also, the study reveals an emerging herd immunity among young men aged 15–19. The decrease in AGW 2008–2011 cannot be explained by behaviour change alone, as the decrease is significantly more pronounced than the decrease found in the chlamydia incidence.
The study also shows a relationship between AGW incidence and relatively low vaccination coverage (up to 20%), which is seen among women aged 20–24. The decrease is significant in itself, and statistically more pronounced than the decrease in the chlamydia incidence. This is not the case for men aged 20–24. Therefore, the study does not provide the sufficient evidence of herd immunity among men aged 20–24.
ACKNOWLEDGEMENT
Conflicts of interest: KK has received fees as a speaker and obtained research grants form Sanofi Pasteur MSD.
References


