


Ken Washio1, Atsushi Fukunaga1*, Minako Terai1, Kiyotaka Hitomi2, Kiyofumi Yamanishi3 and Chikako Nishigori1
1Division of Dermatology, Department of Internal Related, Kobe University Graduate School of Medicine, 7-5-1 Kusunoki-cho, Chuo-ku, Kobe 650-0017, 2Department of Basal Medicinal Sciences, Graduate School of Pharmaceutical Sciences, Nagoya University, Nagoya, and 3Department of Dermatology, Hyogo College of Medicine, Nishinomiya, Hyogo, Japan. *E-mail: atsushi@med.kobe-u.ac.jp
Accepted Aug 15, 2013; Epub ahead of print Oct 24, 2013
Bathing suit ichthyosis (BSI) is a rare variant of autosomal recessive lamellar ichthyosis (LI). In 2005, Jacyk first reported 13 cases of LI that presented with the characteristic distribution of lesions on the trunk but usually sparing the extremities and the central face (1). Subsequently, Oji et al. (2) showed that BSI is caused by transglutaminase-1 (TG1) deficiency with heat-dependent TG1 dysfunction. We and colleagues previously reported a case of BSI with summer exacerbation, suggesting the involvement of a temperature-dependent mechanism (3). However, the mechanism of this temperature-dependent exacerbation remained unclear. In people with acquired idiopathic generalised anhidrosis, the occlusion of proximal coiled ducts results in severe heat intolerance (4). This phenomenon led us to hypothesise that seasonal exacerbation might be associated with hypohidrosis in BSI cases. In this study, we demonstrated that hypohidrosis plays a crucial role in the heating spiral.
CASE REPORT
A 27-year-old man came to our dermatology department with generalised scales. Born a collodion baby, he had always suffered from ichthyosis. His symptoms worsened in summer and improved in winter. Physical examination revealed brownish lamellar scales exhibiting the characteristic “bathing suit” pattern (Fig. 1a). Genetic testing detected compound heterozygous mutations of TGM1. The mutations c.430G>A and c.919C>T led to p.G144R and p.R307W of TG1 in skin specimens taken from his severe and mild lesions, as previously reported (3). Fluorescence assay using FITC-pepK5 (5), a substrate specific to the TG1 enzyme, showed that the in situ TG1 activity was lower on the patient’s lesional skin at 37°C and at 42°C than on the skin of healthy controls, but that the activity showed little change on the patient’s lesional skin between 37°C and 42°C (data not shown).
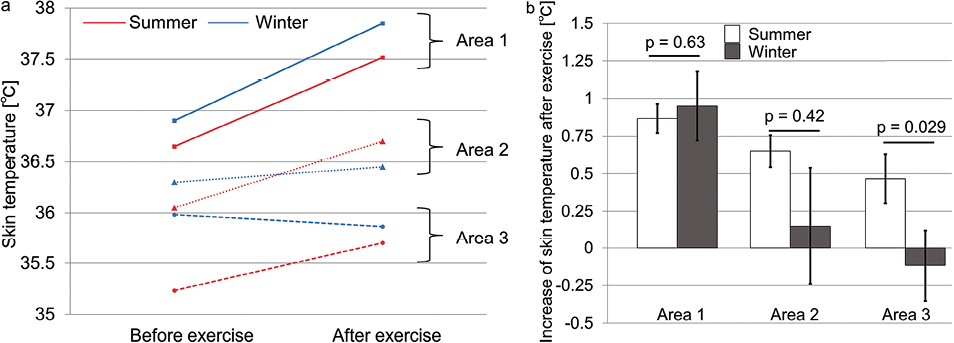
During follow-up over the next few years, we noticed that the patient’s skin could be categorised into 3 areas: area 1 always exhibited lamellar scales; area 2 appeared to exhibit lamellar scales only in summer, and to improve in winter; and area 3 appeared to be normal. Since the patient’s general thermoregulatory sweat test showed severe hypohidrosis (Fig. 1b), we focused on the sweating ability of the patient’s lesional skin. To clarify the differences among these 3 areas, local sweat testing was performed. For this test, the patient’s local skin was painted by topical 1% iodine solution. The sweat glands were stimulated by intradermal injection (0.1 ml) of 100 µg/ml acetylcholine, and the number of perspiration points was assessed based on the picture by the use of Image J software (National Institutes of Health). In area 1, no sweating was detected in summer or winter (Fig. 1c and d), while in area 2 sweating ability improved in winter compared with summer (Fig. 1e, f). In area 3, a small amount of sweat was observed in summer and sweating increased in winter (Fig. 1g, h). We also assessed the surface temperature and the dynamic state of local heat accumulation after treadmill exercise using thermography and a non-contact thermometer (NEC avio, Japan). In summer and winter, skin temperature pre- and post-exercise tended to be higher in areas with hypohidrosis than in perspiring areas (Fig. 2a). The increase in skin temperature, which was observed after exercise in all areas in the summer, was highest in area 1 and lowest in area 3. In winter, the post-exercise skin temperature decreased in area 3 and showed minimal change in area 2 (Fig. 2b).
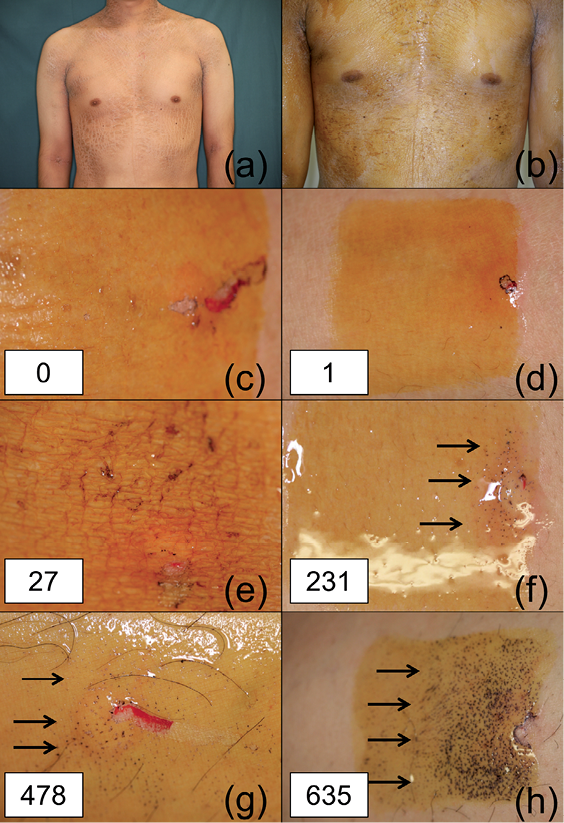
Fig. 1. Clinical findings of the patient. (a) Severe ichthyosis on the trunk. (b) Decreased sweating on general sweat test. (c, e, g) Acetylcholine sweat test results in summer. (d, f, h) Acetylcholine sweat test results in winter. (c, d) The patient’s forearm (area 1). (e, f) The patient’s abdomen (area 2). (g, h) The patient’s leg (area 3). Area 1 (severe ichthyosis is always present), area 2 (ichthyosis appears only in summer, but not in winter), and area 3 (no apparent skin changes). The number of perspiration points was described in white boxes (c–h) and arrows indicate the points.
Fig. 2. (a) Skin surface temperature before and after exercise stress test in summer and winter, respectively. Areas 1–3 are defined in Fig. 1 and in the text. (b) Increase in skin temperature after exercise stress test. Student’s paired t-test; p < 0.05 was considered significant.
DISCUSSION
The characteristic distribution of BSI lesions is explained by the fact that mutant TG1 activity is impaired by heat and restored somewhat at lower temperatures (2, 6). The distinctive feature of our case is the lesional distribution as well as the association with summer exacerbation. Because sweating did not improve in winter in area 1, where the patient had persistent scaly eruptions, the skin temperature showed the same exercise-related increase in summer as in winter. In contrast, increased sweating in winter resulted in minimally increased post-exercise skin temperature in area 2, where the scales seasonally improved. These findings demonstrate that hypohidrosis results in further heat accumulation after exercise. Oji et al. (2) showed that BSI is caused by TG1 deficiency with heat-dependent TG1 dysfunction. In this study, a correlation between hyperkeratotic lesions and hypohidrosis as well as skin temperature has been observed, which suggests that the negative effect of higher temperature on the residual enzyme function might be promoted by associated hypohidrosis. Thus, we hypothesised that heat accumulation leads to additional reduction of TG1 activity, which might result in further hyperkeratosis. However, such further reduction of TG1 activity could not be confirmed because of the minimal fluorescence of natural TG1 activity in this case. Haenssle et al. (7) reported a case of recessive congenital LI in which severe generalised hypohidrosis markedly improved after oral treatment with retinoids, indicating that excessive keratinisation seems to provoke hypohidrosis in patients with LI. In the TG1-deficient patient with BSI exhibiting seasonal exacerbation, we speculate that hypohidrosis following excessive keratinisation results in heat accumulation, which possibly causes additional hyperkeratosis in the summer. This vicious circle may contribute to the seasonal variation in our case.
The authors declare no conflict of interest.
REFERENCES

