


Marléne Isaksson, Inese Hauksson, Monica Hindsén, Ann Pontén, Cecilia Svedman and Magnus Bruze
Department of Occupational and Environmental Dermatology, Skåne University Hospital, Lund University, Malmö, Sweden
The preservative methylchloroisothiazolinone/methylisothiazolinone (MCI/MI) is a well-known sensitiser and present in most baseline series since at least 20 years. The proportions of MCI/MI are 3:1. MI alone has been used as a preservative in occupational and household products, and cosmetics since less than 10 years. MCI/MI tested at 100 ppm fails to detect a significant percentage of contact-allergic reactions to MI. Our aim was to investigate whether a separate test preparation with MI picks up additional cases of contact allergy to MI not detected with MCI/MI 200 ppm. MI was inserted into the baseline series of the Malmö clinic in 2003 starting at 475 ppm, then 900 ppm, then 1,000 ppm, 1,500 ppm and finally 2,000 ppm. In 5,881 consecutively tested dermatitis patients the contact allergy rate for MI varied between 0.5 and 6.5%, with a marked increase in recent years. The contact allergy rate to MI 2,000 ppm alone, not traced by MCI/MI 200 ppm, varied between 0 and 1.9%. In conclusion, due to the increase of contact allergy to MI not traced by MCI/MI 200 ppm, MI in water at 2,000 ppm should be tested in a baseline series. Independent of patch test technique a dose of 60 µg/cm2 should not be exceeded to avoid adverse reactions and particularly patch test sensitisation. Key words: contact allergy; patch testing; methylchloroisothiazolinone/methylisothiazolinone 3:1 CAS 55965-84-9; methylchloroisothiazolinone CAS 26172-55-4; methylisothiazolinone CAS 2682-20-4; Kathon CG; dose in µg/cm2; micropipette; patch test sensitisation; preservative.
Accepted Mar 11, 2014; Epub ahead of print Mar 25, 2014
Acta Derm Venereol
Marléne Isaksson, Department of Occupational and Environmental Dermatology, Skåne University Hospital, SE-205 02 Malmö, Sweden. E-mail: marlene.isaksson@med.lu.se
The preservative methylisothiazolinone (MI) has been used in industry since the early 2000 in non-regulated concentrations and in cosmetics and toiletries since 2005 at a maximal allowed concentration of 100 ppm. Also household products such as detergents and abrasive creams contain this preservative. We published the first 2 cases of occupational allergic contact dermatitis from MI in 2004 (1) but the first cases of contact allergy to MI were demonstrated already in 1987, when patients detected with methylchloroisothiazolinone/methylisothiazolinone (MCI/MI) contact allergy were tested to the 2 active ingredients (a.i.) separately (2). To monitor the contact allergy frequency among our dermatitis patients we included MI into our baseline series in 2003. This article aims at describing the frequency of MI contact allergy and the simultaneous reactions to MCI/MI in our tested dermatitis patients from 2003 up until 2013.
MATERIALS AND METHODS
Study period
The study period is from March 17, 2003 until 31 December 2012 with an intermission from February 4, 2010 until June 30, 2011, when MI was tested in our paint series and not in the baseline series.
Patch-test preparations
The Swedish baseline series was purchased from Chemotechnique Diagnostics, Vellinge, Sweden. The following biocides were used: (i) Kathon CG (formerly Rohm and Haas Company, Philadelphia, PA, USA; now The Dow Chemical Company, Midland, Michigan, USA), which consists of the a.i. MCI (1.125%) and MI (0.375%); (ii) Neolone 950, (formerly Rohm and Haas, now The Dow Chemical Company), which contains water and MI at 950 ppm, according to its material safety data sheet. In our baseline series, it was first tested at a concentration of 475 ppm, then at 950 ppm, then at 1,000 ppm, 1,500 ppm and finally at 2,000 ppm (Table SI1).
Patch testing
Patch testing was performed using Finn Chambers® (Ø 8 mm) (Epitest Ltd Oy, Tuusula, Finland) secured with Scanpor® tape (Norgesplaster A/S, Vennesla, Norway). Fifteen microlitres of each test solution were micropipetted on to the filter paper discs (3). Tests were left on the upper back for 48 h and readings according to the International Contact Dermatitis Research Group criteria took place on day (D) 3 and 7 (4).
Neolone 950 0.5% aqua (corresponding to 475 ppm MI) was inserted into the baseline series on March 17, 2003, where MCI/MI 0.02% (200 ppm; MCI 150 ppm, MI 50 ppm) aqua has been present since 1985. The concentration of Neolone 950 was increased to 1.0% aqua (950 ppm MI) on April 25, 2003, as we had not seen any cases suspected of patch test sensitisation or irritant reactions. From October 1, 2005, the concentration of Neolone 950 was increased to 1,000 ppm, which was tested until December 31st, 2006. From January 1st–December 31st, 2006, Neolone 950 at 1,500 ppm was tested in parallel. The test concentration was raised to 2,000 ppm on January 1st 2007 until December 31 2012 with an intermission during one and a half year (2010-02-04–2011-06-30).
Statistics
The Fisher’s test (two-sided) was used to compare the outcome of contact allergy to MCI/MI and MI, respectively, in males and females. A p-value < 0.05 was considered significant.
RESULTS
Test results are shown in Table SI1. Test results from D3 and D7 are compiled into either positive or negative reactions. In total, 5,899 dermatitis patients (2,222 men and 3,677 women) were patch-tested to MCI/MI 200 ppm in the baseline series during the study period. During the same time, 5,881 patients (2,216 men and 3,665 women) were patch-tested to the various concentrations of MI.
During the whole test period 184 patients (3.1%) reacted to MCI/MI 0.02% aqua. The contact allergy frequencies to MCI/MI varied between 1.8 to 3.0% between the years 2003–2009. Since 2010 an increase is seen, from 4.3% in 2010 to 7.6% in 2012 (Table SI1, Fig. 1).
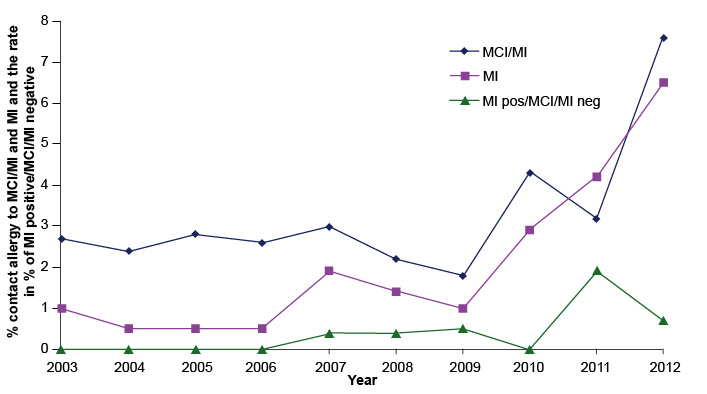
Fig. 1. The contact allergy frequencies of MCI/MI and MI during the years 2003–2013 and the rate of MI positive/MCI/MI negative in percent. MCI/MI tested at 200 ppm; MI tested at 475 ppm from March 2003–April 2003; 950 ppm from May 2003–September 2005; 1,000 ppm from October 2005–December 2006; 1,500 ppm from January 2006–December 2006; 2,000 ppm from January 2007–December 2012.
MI contact allergy varied during 2003–2009 between 0.5 and 1.9%. From 2003 until 2007 MI was tested at 4 different concentrations. MI tested at 475 ppm had a contact allergy rate of 1.0%. For MI tested at 950, 1,000, and 1,500 ppm the figure was 0.5%. From 2007 MI 2,000 ppm was tested and the frequencies varied from between 1.0 to 1.9%. From 2010 an increase was noticed from 2.9% in 2010 to 6.5% in 2012 (Table SI1, Fig. 1). The number of MI-allergic cases not traced with the MCI/MI preparation 200 ppm rose from 0% during the years 2003–2006, when MI was tested at 475, 950, 1,000 and 1,500 ppm, to 0.4–0.5% during the years 2007–2010, when MI was tested at 2,000 ppm. From 2011 an increase to 1.9% was seen and in 2012 the figure was 0.7% (Table SI1, Fig. 1).
Of the 101 patients reacting to any concentration of MI in the baseline series, 19 (19%) did not react positively to MCI/MI 200 ppm. Of the 184 patients reacting to MCI/MI 200 ppm in the baseline series, 80 were simultaneously reacting to MI.
There were no significant differences between males and females in the contact allergy frequencies to MI during the whole test period irrespective of patch test concentration although a female predominance, not reaching statistical significance (p = 0.063), was seen. Concerning MCI/MI, for the whole period a female predominance not reaching statistical significance was seen (p = 0.063), except for the year 2012, when a significant difference was seen for females compared to males (p = 0.022).
DISCUSSION
Until about 10 years ago our patients have been simultaneously exposed to MCI and MI, as these always have been present together in various products, except in those cases where the MCI part had been consumed due to high pH and/or presence of sulphur-containing proteins (unpublished observations). Patch testing with the combination MCI/MI has been the gold standard to detect contact allergy to preservatives containing the 2 a.i. In Europe, however, a biocide containing exclusively MI without MCI has been on the market since the early 2000 for industrial use and since 2005 in cosmetics and toiletries. To monitor the contact allergy frequency in our dermatitis patients we inserted Neolone 950 into our baseline series already in 2003. Initially we tested with MI 475 ppm but soon increased the concentration and since 2007 we test with MI 2,000 ppm. The frequency of contact allergy to MCI/MI has been stable, around 2–3% during the years 2003–2009. The frequency of contact allergy to MI has been around 0.5–1.5% during the same period. Simultaneous contact allergy to MI was seen in over 80% of our MCI/MI-hypersensitive patients. This figure is higher than other published data. In Denmark concomitant positive patch test reactions to MI and MCI/MI were found in 41% of their MI-allergic patients (5) and in Germany the proportion of MI-positive patients among those reacting to MCI/MI increased from 43% to 59% between 2009 and 2011 (6). One reason our figure is higher may be the fact that in Sweden we patch test MCI/MI at 200 ppm instead of 100 ppm (7). We know that 100% more contact allergies are detected with 200 compared to 100 ppm (8). We also always use a micropipette when we apply liquid test preparations and use the set volume 15 µl when we use the Finn chamber technique with a diameter of 8 mm to get an exact dose, i.e. the dose 0.006 mg/cm2 MCI/MI. In the patients that reacted to both MCI/MI and MI, the explanation to the MI reaction were in the majority of cases cross-reactivity due to primary MCI/MI sensitisation and thus subsequent MCI sensitisation and cross-reactivity to MI. This has been shown in 2 human studies in which patients sensitised to MCI/MI were patch-tested to both the a.i. separately and where all patients tested positively to MCI and the majority negatively to MI (2, 9). In one of the articles where workers had been occupationally sensitised to MCI/MI, one tested positively to MI but in this case, there was a 7 times higher reactivity to MCI than to MI. In that article we concluded that the most likely explanation was a cross-reaction between MCI and MI (9).
The banning of methyldibromo glutaronitrile in cosmetics by the EU has resulted in a come back of the strong allergenic mixture of MCI/MI (5, 10, 11). MI alone has recently been introduced in cosmetics to replace the mixture MCI/MI, since it is less allergenic. However, it is also less active, so higher concentrations are needed for preservation. With a widespread use of this weak/moderate sensitiser (12–14) in higher concentrations a rise in contact allergy to MI is currently being observed in most European countries. The highest rates have so far been reported from the UK where an increase has been noticed in Leeds from 0.6% in 2009 (MI then tested at 200 ppm) to 4.6% in 2012 (MI tested at 2,000 ppm since 2011) (11) and from Amersham from 2.5% in 2009 to 9.2.% in 2012 (MI then tested at 500 ppm) and in the first 6 months of 2013 to 10.8% (MI tested at 2,000 ppm) (personal communication David Orton, U.K.). A male predominance has been reported from the UK (personal communication David Orton, U.K.), Denmark (5), Germany (15), and Sweden (16). However, in this present study encompassing all the investigated years there is no significant male predominance neither for MI nor for MCI/MI.
In our clinic, from 2010, the frequency of contact allergy to MI has also risen and is paralleled by MCI/MI (Fig. 1). In 2010, 2.9% reacted to MI, in 2011 a sharp increase to 4.2% was seen and in 2012 an even higher frequency was seen, i.e. 6.5%. The frequencies for MCI/MI were during the same period 4.3, 3.2, and 7.6%, respectively. Furthermore, the number of missed cases of contact allergy to MI when only patch testing to MCI/MI 200 ppm has also increased from 0.4% in 2007 to 0.7 in 2012 with a peak in 2011 at 1.9%. The same observation has been made recently in many countries in Europe, where the number of additional cases with contact allergy to MI traced by the testing with MI simultaneously with the testing of MCI/MI at 200 ppm or 100 ppm in a baseline series varies between 0 and 1.6% for 200 ppm (11, 16) and 0.5 and 0.8% for 100 ppm (5, 17, 18). In 2 German reports on aimed testing with MI the additional contact allergy to MI excluding those with a simultaneous contact allergy to MCI/MI 100 ppm is 0.5% and 1.2%, respectively (6, 15).
In a recent publication on MI (18) it was discussed why the increase in incidence of contact allergy to MI (5, 10, 11, 15–17) has happened, and it was concluded that it probably could be explained by the fact that the use of cosmetics preserved with MI has increased (19, 20) and that a substantial proportion contains more than 10–20 ppm (19).
Currently, the occupational exposure seems to be predominated by MI in paints (21, 22) while the non-occupational exposure to MI in cosmetics and household products is prevailing. Individual cases with allergic contact dermatitis from MI have been reported from a waist reduction belt (23), in painters (1, 19), from cosmetics and wet wipes for intimate hygiene or baby-care (24), from hair cosmetics, facial cosmetics (5, 19), deodorants (25) and sunscreens (20). Even airborne allergic contact dermatitis and systemic contact dermatitis have been attributed to MI release from recently painted walls (26–28), or from a toilet cleaner (29). If contact allergy to MI is demonstrated and there is a strong suspicion that the patient is exposed to MI but the information from the manufacturer is misleading, chemical investigation of the product is possible. Recently such a case was observed in Belgium (30).
MI at 2,000 ppm has recently been included into the European baseline series (18). The same test preparation of MI will also be included in the Swedish baseline series from 2014 to detect cases with allergic contact dermatitis from MI and to follow the trends also in Sweden. To stop the trend we see all over Europe, action against the high use concentrations of MI in cosmetics and industrial products such as paints should be undertaken and an initiative has already been conducted by the European Society of Contact Dermatitis. However, care should be taken by legislative bodies so that we do not get new even more allergenic preservatives in the environment than we already have or that the use of “old” allergenic preservatives is increased, both in volume and in use concentrations, such as we have seen now with MI and MCI/MI after the banning of methyldibromo glutaronitrile.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1844
References


