


Josep Malvehy1–3, Rodrigo Roldán-Marín1,4, Pablo Iglesias-García1, Alba Díaz5 and Susana Puig1–3
1Melanoma Unit, Dermatology Department, Hospital Clínic, 2Institut d’Investigacions Biomèdiques August Pi I Sunyer (IDIBAPS), 3Centre on Biomedical Research on Rare Diseases (CIBERER), Instituto Carlos III, 4Almirall S.A., Global Dermatology Business Unit, and 5Pathology Department, Hospital Clínic, Barcelona, Spain
Visual inspection may fail to accurately evaluate field cancerisation (subclinical actinic keratoses [AKs]). We aimed to describe field cancerisation by confocal reflectance microscopy and changes induced by the application of 3% diclofenac sodium gel in 2.5% hyaluronic acid. Fourteen male patients, > 50 years old, with AKs on the bald scalp were included. Clinical examination, confocal microscopy and histological study of clinically visible lesions and “normal appearing” adjacent skin before and after treatment was completed. Reflectance confocal microscopy showed a decrease in scaling (p = 0.001) and atypia of the honeycomb pattern (p = 0.001) at 2 weeks of treatment. Changes in parakeratosis, inflammation and dermal collagen remodelling were also observed. Histology correlated with confocal features in AK and subclinical AK. Reflectance confocal microscopy was useful in the evaluation of field cancerisation and monitoring of treatment response. A rapid improvement in epidermal atypia was observed. Key words: field cancerisation; actinic keratosis; reflectance confocal microscopy; histology; diclofenac; hyaluronic acid.
Accepted Apr 1, 2014; Epub ahead of print Apr 3, 2014
Acta Derm Venereol
Dr. Josep Malvehy, Melanoma Unit, Dermatology Department, Hospital Clínic, C/Villarroel, 170, ES-08036 Barcelona, Spain. E-mail: jmalvehy@gmail.com
In the skin, “field cancerisation” (1, 2) describes subclinical lesions with “normal appearing skin” surrounding clinically visible actinic keratosis (AK), providing the basis for clonal expansion of genetically altered neoplastic cells (1–5). The diagnosis of AK is generally based on clinical examination. However, biopsy and histological evaluation are performed in clinically indistinct cases, or if invasive squamous cell carcinoma (SCC) is suspected. While visual inspection may fail to detect early subclinical changes, repeated invasive histological analysis of areas with extensive actinic damage often may not be feasible.
AKs are commonly present in areas of chronic actinic damage. Histologically, AKs have been classified according to keratinocyte atypia, nuclear pleomorphism, hyperkeratosis, parakeratosis, a dermal inflammatory infiltrate and concomitant solar elastosis (6). AK is one stage of a biologic continuum in the progression from subclinical keratinocyte dysplasia to invasive SCC (7–12). However, in the clinical setting, patients often present with numerous AKs at various stages of graded differentiation and the extent of subclinical disease is difficult to determine.
In thinking about the various diagnostic modalities currently available, it is clear that a diagnosis based on clinical grounds alone may not be sufficiently reliable, while the feasibility of obtaining biopsies of all affected sides and surrounding skin is limited. Hence, in recent years interest has risen in the development of novel non-invasive diagnostic techniques that not only allow precise diagnosis of clinical AKs but also allow detection and definition of subclinical disease. In vivo reflectance confocal microscopy (RCM) generates horizontal skin sections with quasi-histological resolution. Its use in the detection of AKs and field cancerisation, as well as the evaluation of response to topical treatments has been clearly established (5, 13–16).
Several new therapeutic options have become available over recent years, and there remains debate about the best treatment options for AKs and field cancerisation. Treatment options for AKs include a wide range of ablative modalities and topical treatments such as diclofenac sodium gel, imiquimod, ingenol mebutate gel or 5-fluorouracil with salicylic acid. Diclofenac sodium 3% gel is a non-steroidal anti-inflammatory topical agent that demonstrates preferential inhibition of cyclo-oxygenase-2 (COX-2), an enzyme implicated in ultraviolet (UV)-induced skin carcinogenesis (17–27). The treatment of AKs with topical 3% diclofenac in 2.5% hyaluronic acid (Solaraze®, Almirall, S.A., Barcelona, Spain) has been extensively documented in the last decade (17). However, precise information regarding in vivo morphological changes induced by this drug in the skin is needed. In the present study we aimed to describe the changes in the skin of patients with clinical and subclinical AK during and after topical treatment with 3% diclofenac sodium with 2.5% hyaluronic acid by RCM, and describe the correlation between RCM and histology. The study was not designed to assess clinical response or to compare this drug with other alternatives but to demonstrate the changes in vivo induced by the drug.
MATERIAL AND METHODS
Twenty volunteer male patients, aged >50 years old, Fitzpatrick’s skin phototype I–III, with a minimum of 3 clinically visible AK on the bald scalp, were included in this study. Written informed consent was obtained from each participant before evaluation. Evaluation consisted of clinical examination, dermoscopic imaging and RCM evaluation of a clinically visible AK and “normal appearing” adjacent skin. In each participant, lesions clinically diagnosed as AK were selected for imaging and biopsy as well as adjacent, apparently unaffected skin. An area of 2 × 2 cm on the scalp including at least 3 AK was selected. At the first visit, a 3-mm punch biopsy was performed in one AK and another 3-mm punch biopsy was performed in normally apparent surrounding skin (subclinical AK) (Fig. 1). Additionally, one clinical AK and one subclinical AK were also selected at baseline (t1) to be biopsied at the end of the treatment (t4). Transparency body charts were used to outline the selected skin areas at baseline and to permit co-localisation. Highlighted skin areas were documented on the chart by using permanent marker pens in a colour-coded fashion, correlating individual colours to selected evaluation dates. Evaluation with reflectance confocal microscopy was performed before treatment (time 1), at week 2 (time 2), at week 6 (time 3), at end of treatment (time 4) in 4 sub-areas (8 × 8 mm) inside the selected 2 × 2 cm area. Sites of biopsies at t1 were avoided for the RCM evaluation.
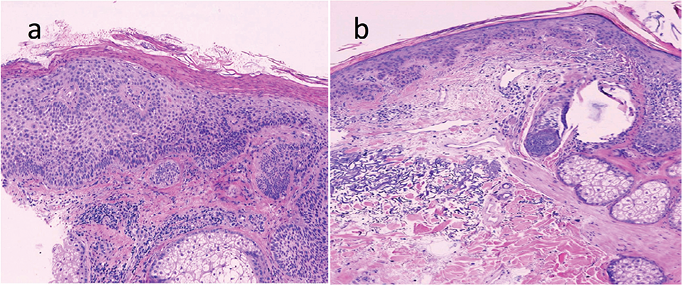
Fig. 1. Actinic keratosis (a) and subclinical actinic keratosis (b) by routine histology (H&E) (× 100). Presence of parakeratosis, architectural disarray, keratinocyte atypia seen to a varying degree.
Following the approved indication treatment with topical diclofenac sodium 3% in 2.5% hyaluronic acid was applied twice daily for 90 days over the affected skin area, covering both clinically affected AKs and apparently unaffected adjacent skin.
A commercially available in vivo reflectance confocal microscope (Vivascope 1500, Lucid-Tech, Inc., Henrietta, NY, USA; MAVIG GmbH, Munich, Germany) was used to image AKs and surrounding “normal appearing” skin. A detailed description of the technique and the device has been published previously (13–15). For each skin site analysed, systematic horizontal mapping was performed and 4–8 images were captured in axial sections beginning with the stratum corneum, through the entire epidermis and into the upper reticular dermis using the “Vivablock” function modality (each vivablock was 16 × 16 = 254 images composite). Furthermore, a vertical mapping using the “Vivastack” was performed in 5 µm steps to a maximum depth of 200 µm beginning with the stratum corneum through the entire epidermis and into the superficial dermis. RCM images were individually subjected to evaluation.
Diagnostic reflectance confocal microscopy (RCM) criteria for AK are shown in Table SIa1.
Diagnostic criteria for AK included parakeratosis, hyperkeratosis, individual detached keratinocytes, architectural disarray, keratinocyte atypia and pleomorphism as shown in Table SI1.
An investigator obtained images of all test sites (RR). The corresponding RCM images were then subject to blinded evaluation by 2 independent experts in the field of confocal microscopy (JM and SP). Evaluators were blinded to participant’s name, age and treatment duration.
Skin punch biopsies (4 mm in diameter) were obtained under sterile conditions after local anaesthesia with lidocaine 1% from a previously selected skin lesion clinically diagnosed as AK, and also from apparently unaffected adjacent skin at t1 and end of treatment (t4). The skin samples were fixed in 10% formalin and processed by routine histopathology. Staining with haematoxylin and eosin was performed and slides were evaluated by a board-certified pathologist (AD). Immunohistochemical stains were performed to evaluate COX-2 expression, p53 mutation, Ki67, PCNA, p21 and CD31 before and at the end of treatment. The histopathological and immunohistochemical scores used are detailed in Table SIb1.
Statistical analysis
The statistical analyses for categorical variables were performed with a chi-squared test, or Fisher’s test for 2 × 2 tables when required depending on the sample size. For continuous variables; the mean score for each parameter before treatment (t1; histology or RCM) was compared with the mean score during (t2, t3, RCM) and at the end of the study (t4; histology and RCM) using Student t-test for paired samples for normally distributed data. ANOVA was used for multiple comparisons at different times (t1, t2, t3, t4).
RESULTS
At the end of the study 14 patients were able to complete the treatment course and evaluation. Six patients dropped out of the study. Two patients withdrew consent and did not follow-up with treatment or evaluation after inclusion (t1). Four patients were excluded from the study during the treatment course because they were unwilling to continue with treatment or follow-up due to local adverse skin reaction to the topical application of 3% diclofenac sodium with 2.5% hyaluronic acid. These local adverse events consisted mainly of moderate to severe erythema, mild to moderate scaling, dryness and pruritus.
A total of 59,136 RCM images were obtained. The presence of scaling, the area of atypical honeycomb and the degree of atypical honeycomb decreased after 2 weeks of treatment (p = 0.001; p = 0.002; p = 0.000). These changes persisted after the end of treatment (p = 0.000 for all 3) (Fig. 2). After 2 weeks of treatment, the presence of polygonal nucleated cells, detached individual corneocytes and inflammation increased (p = 0.003, p = 0.004; p = 0.002) (Table SII1) (Figs 3 and 4). These increases in polygonal nucleated upper cells and detached corneocytes were normalised at the end of treatment (p = 0.696; p = 0.311) (Table SII1). On the contrary, an elevated level of inflammation persisted during the entire period of study (p = 0.025) showing the presence of small bright inflammatory cells and some dendritic cells in the spinous cell layer as well as in the upper dermis (Fig. 4). Changes in dermal collagen thickening and arrangement of fibres in the upper dermis were observed at the end of treatment (Fig. 5). Huddles of collagen and curled fibres, that have been described in elastosis, were replaced by aligned thinner fibres.
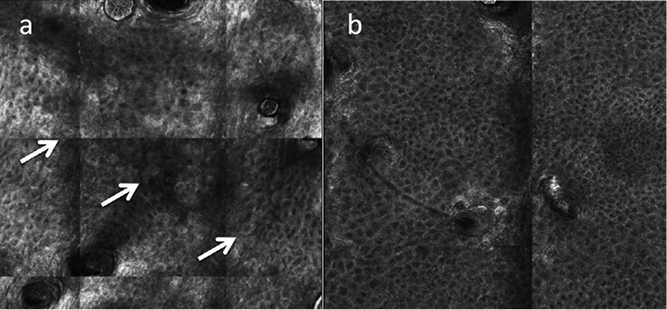
Fig. 2. Reflectance confocal microscopy (RCM) image (vivablock 1.2 mm2) with atypical honeycomb in the stratum spinosum of a subclinical actinic keratosis at time 0 before treatment (a). Presence of atypical keratinocytes with irregular size, shape and refractivity (white arrows). On the right image (b) RCM of the same lesion after the treatment at time 4. Normalisation of honeycomb pattern in the same lesion is clearly seen.
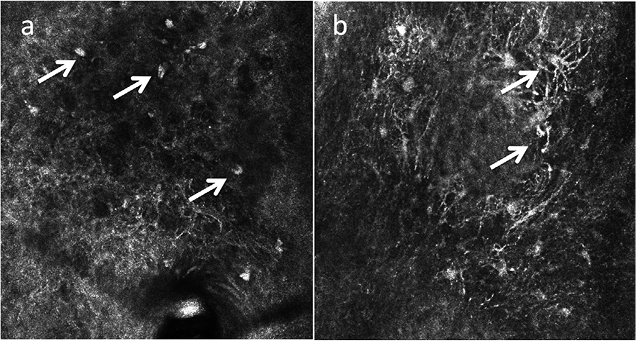
Fig. 4. Presence of inflammatory cells (white arrows) at time 2 of treatment in subclinical actinic keratosis seen under reflectance confocal microscopy in the stratum spinosum of the epidermis (0.5 × 0.5 mm) with round nucleated cells corresponding to lymphocytes (a) and dendritic cells corresponding to Langerhans’ cells (b).
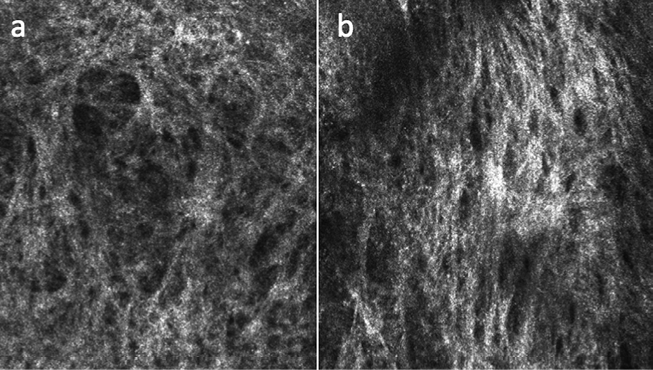
Fig. 5. Reflectance confocal microscopy image of the upper dermis showing changes in the collagen in a subclinical actinic keratosis before treatment at time 0 (a) and after treatment at time 4 (b). Huddles of collagen and curled fibres, corresponding to elastosis are replaced by aligned thinner fibres.
Histology before and after the treatment course showed an important reduction in epidermal atypia in AK (p = 0.001) and subclinical AK (p = 0.003) between t1 and t4. Immunohistochemical analysis demonstrated a reduction in cellular proliferation measured by the expression of Ki67 in AK (p = 0.02) and subclinical AK (p = 0.023) at the end of treatment. In subclinical AKs, there was a marked reduction in the expression of the vascular marker CD31 (p = 0.017) after treatment. Evaluation of COX-2 expression was available in just 7 paired AK and 7 paired subclinical AK samples (t1–t4) decreasing significantly in AK (p = 0.047) but just showing a tendency to decrease in subclinical AK (p = 0.078) (Table I).
Table I. Comparison of immunohistopathological findings in actinic keratosis and subclinical actinic keratosis lesions at baseline and at the end of treatment
|
Actinic keratosis |
Subclinical actinic keratosis |
|||||||||||
|
Mean |
n |
Deviation typical |
Error typical of the mean |
p-value |
Mean |
n |
Deviation typical |
Error typical of the mean |
p-value |
|||
|
Epidermal thickness |
t1 |
0.90 |
10 |
0.876 |
0.277 |
0.25 |
0.40 |
10 |
0.516 |
0.163 |
0.081 |
|
|
t4 |
0.20 |
10 |
0.422 |
0.133 |
0.10 |
10 |
0.316 |
0.100 |
||||
|
Thickness of stratum corneum |
t1 |
1.60 |
10 |
0.516 |
0.163 |
0.19 |
0.80 |
10 |
0.632 |
0.200 |
0.394 |
|
|
t4 |
0.70 |
10 |
0.675 |
0.213 |
1.10 |
10 |
0.738 |
0.233 |
||||
|
Epidermal atypia |
t1 |
2.00 |
10 |
0.000 |
0.000 |
0.001 |
1.70 |
10 |
0.483 |
0.153 |
0.003 |
|
|
t4 |
1.30 |
10 |
0.483 |
0.153 |
0.90 |
10 |
0.568 |
0.180 |
||||
|
Thickness of atypia |
t1 |
1.40 |
10 |
0.516 |
0.163 |
0.037 |
1.00 |
10 |
0.000 |
0.000 |
0.168 |
|
|
t4 |
1.00 |
10 |
0.000 |
0.000 |
0.80 |
10 |
0.422 |
0.133 |
||||
|
Inflammation |
t1 |
1.20 |
10 |
0.632 |
0.200 |
0.168 |
0.40 |
10 |
0.516 |
0.163 |
0.509 |
|
|
t4 |
0.80 |
10 |
0.422 |
0.133 |
0.60 |
10 |
0.516 |
0.163 |
||||
|
Type of inflammation |
t1 |
0.90 |
10 |
0.316 |
0.100 |
0.591 |
0.40 |
10 |
0.516 |
0.163 |
0.509 |
|
|
t4 |
0.80 |
10 |
0.422 |
0.133 |
0.60 |
10 |
0.516 |
0.163 |
||||
|
ki67 |
t1 |
3.00 |
9 |
0.000 |
0.000 |
0.02 |
2.60 |
10 |
0.699 |
0.221 |
0.023 |
|
|
t4 |
1.78 |
9 |
0.833 |
0.278 |
1.60 |
10 |
0.966 |
0.306 |
||||
|
PCNA basal |
t1 |
2.67 |
9 |
0.500 |
0.167 |
0.169 |
2.44 |
9 |
0.527 |
0.176 |
0.347 |
|
|
t4 |
2.22 |
9 |
0.667 |
0.222 |
2.22 |
9 |
0.667 |
0.222 |
||||
|
PCNA suprabasal |
t1 |
3.00 |
9 |
0.000 |
0.000 |
0.169 |
3.00 |
9 |
0.000 |
0.000 |
0.081 |
|
|
t4 |
2.78 |
9 |
0.441 |
0.147 |
2.67 |
9 |
0.500 |
0.167 |
||||
|
p53 basal |
t1 |
2.00 |
10 |
0.943 |
0.298 |
0.244 |
1.70 |
10 |
0.483 |
0.153 |
0.591 |
|
|
t4 |
1.50 |
10 |
0.850 |
0.269 |
1.50 |
10 |
0.972 |
0.307 |
||||
|
p53 supra basal |
t1 |
2.20 |
10 |
0.632 |
0.200 |
0.193 |
2.30 |
10 |
0.949 |
0.300 |
0.087 |
|
|
t4 |
1.90 |
10 |
0.738 |
0.233 |
1.50 |
10 |
0.972 |
0.307 |
||||
|
p21 suprabasal |
t1 |
1.56 |
9 |
0.527 |
0.176 |
0.193 |
1.20 |
10 |
0.789 |
0.249 |
0.758 |
|
|
t4 |
1.22 |
9 |
0.441 |
0.147 |
1.30 |
10 |
0.675 |
0.213 |
||||
|
CD31 |
t1 |
28.67 |
9 |
16.815 |
5.605 |
0.103 |
31.40 |
10 |
13.251 |
4.190 |
0.017 |
|
|
t4 |
18.89 |
9 |
4.781 |
1.594 |
19.80 |
10 |
8.176 |
2.585 |
||||
|
COX-2 |
t1 |
1.29 |
7 |
1.113 |
0.421 |
0.047 |
1.00 |
7 |
0.816 |
0.309 |
0.078 |
|
|
t4 |
0.57 |
7 |
0.787 |
0.297 |
0.57 |
7 |
0.787 |
0.297 |
||||
DISCUSSION
AK is the most common in situ carcinoma of the skin, the incidence of which is increasing in many world populations (19, 28, 29). The relative risk of SCC increases with the number of AK lesions with an increase from 1% in those with fewer than 5 lesions to 20% in those with more than 20 lesions (30–32). Subclinical (invisible) AKs are estimated to occur up to 10 times more frequently than visible AKs, particularly in sun-damaged skin (33). Currently it is not possible to determine which AK lesion will progress to SCC by clinical or histopathological means (34, 35). Thus, early adequate diagnosis and treatment of all visible and subclinical lesions is recommended to reduce the potential risk of progression to a more advanced disease and possibly invasive and metastatic SCC.
Despite demonstrating itself to be an efficacious treatment of clinically visible AK, even in high-risk organ transplant recipients (17, 27), the effects of 3% diclofenac sodium with 2.5% hyaluronic acid in subclinical lesions (field cancerisation) have not yet been described.
RCM is able to detect field cancerisation changes not only in the AK areas but also in “normal appearing skin” (subclinical AK) by visualisation of atypical honeycomb within the granular and spinous cell layer (17). In the present study, treatment with 3% diclofenac sodium in 2.5% hyaluronic acid was able to improve the epidermal atypia (evaluated as extension of the atypical honeycomb and degree of atypia in the honeycomb) even after only 2 weeks of treatment. This improvement persisted at the end of the study and correlated with the histological evaluation. However, there seemed to be an increased epidermal turnover suggested by the increased presence of detached corneocytes and polygonal nucleated cells in the stratum corneum after 2 weeks of treatment. We hypothesise that these findings may be related to the induction of apoptosis of dysplastic keratinocytes induced by COX-2 inhibition as has been documented in a SCC cell line (22, 23).
RCM revealed the appearance of intraepidermal inflammatory cells during the treatment course. These inflammatory changes were characterised by the presence of some small bright cells and some dendritic cells. We think these findings may be caused by a pro-inflammatory microenvironment where interleukins and chemokines attract leukocytes that “repair” and “clear” the altered keratinocytes as a consequence of the induced apoptosis (18). However, contact dermatitis induced by the drug was not ruled out and the inflammation seen clinically and by RCM could be due to this cause in some patients.
Dermal collagen rearrangement in the superficial dermis was observed after the treatment course. The presence of huddles of collagen and curled fibres were observed previous to the treatment. These findings have been described in skin ageing and correlated with elastosis (36). We hypothesise that our finding of thickened collagen bundles after the end of treatment may be due to the effects of the topical hyaluronic acid stimulating dermal collagen production. Until recently, the hyaluronic acid was thought to serve as a “reservoir” that allowed the 3% diclofenac to accumulate as an intraepidermal depot (37), explaining the sustained clinical clearance of lesions even months after the end of treatment. However, recent data suggest that injected intradermal hyaluronic acid may stimulate dermal collagen production even in aged skin (38).
The immunohistochemical results are in accordance with previous findings that suggest that treatment with 3% diclofenac in 2.5% hyaluronic acid gel causes regression of signs of cancerous transformation and inhibition of atypical keratinocyte proliferation (39). It is noteworthy that despite having a small number of patients the immunohistochemical results in this study showed that at the end of treatment, diclofenac sodium gel in hyaluronic acid was able to significantly modify epidermal atypia in both clinical and subclinical AK. This immunohistochemical finding correlated with the findings by RCM as shown in Fig. 2. Another relevant immunohistochemical result was the significant change in CD31 expression (a marker of angiogenesis) in subclinical AK at the end of treatment. This finding is consistent with previous results from other authors (24, 39) and likely related to the effects of the drug on COX-2 inhibition.
The present study has some limitations due to the small sample size and being a non-randomised, uncontrolled study without long-term follow-up. Although the efficacy of diclofenac to treat AKs has been proven in controlled studies compared to vehicle, and it was not the aim of this study to show clinical response, it is not possible to rule out that some AKs were self-resolving as there was no comparison with a control group. The aim of this study was instead to show the morphological changes in clinical and subclinical AKs by RCM and its histopathological correlation.
RCM may bridge the gap between clinical evaluation and histopathologic evaluation allowing tissue analysis at near cellular resolution that is comparable to routine histology. It is particularly useful to non-invasively monitor treatment response. When evaluating patients with AKs, it provides the added benefit of allowing detection and extension of field cancerisation (subclinical disease).
In conclusion, our findings support the utility of RCM in the evaluation of field cancerisation and monitoring changes during therapy over time. This information may add to our knowledge about the timing and characteristics of changes induced by any therapy.
Acknowledgements
We would like to thank Almirall S.A., for providing the funding to carry out this study. We are also deeply grateful with Dr. Martina Ulrich, for her consultancy in the performance of the COX-2 immunohistochemistries. We also want to express our gratitude to Mrs. Martha Driessen and Mrs. Carolin Meyers, for their invaluable help with editing and proofreading of the manuscript.
Conflicts of interest: Dr. Josep Malvehy has served as a consultant for Almirall, S.A. and MAVIG GmbH. Dr. Rodrigo Roldán-Marín is a part-time employee for Almirall’s Global Dermatology Business Unit. Almirall S.A. provided the funding to carry out this study.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1860
REFERENCES


