


Mingyang Lee1,2, Quan Chen1,2, Huijun Wang1–3, Jie Zhang1,2, Zhimiao Lin1,2 and Yong Yang1–3
1Department of Dermatology, Peking University First Hospital, 2Beijing Key Laboratory of Molecular Diagnosis on Dermatoses, Beijing 100034, and 3Peking-Tsinghua Center for Life Sciences, Beijing, China. E-mail: zhimiaolin@bjmu.edu.cn
Accepted Apr 24, 2014; Epub ahead of print May 7, 2014
Junctional epidermolysis bullosa (JEB) is an autosomal recessive, clinically and genetically heterogeneous disorders (1). A variety of extracutaneous complications may also arise, including gastrointestinal and genito-urinary tract involvements (1, 2). Genito-urinary involvement is particularly common in JEB with congenital pyloric atresia (JEB-PA; MIM 226730) associated with germline mutations in ITGA6 and ITGB4,which encode the α6 and β4 integrin, respectively (2). Recent studies suggested that pylori atresia (PA) was not necessarily a feature of integrin-associated JEB, while urologic problems occur frequently (3, 4). Here, we report a Chinese case with mild ITGB4-associated JEB with profound urinary tract stenosis.
CASE REPORT
The proband was a 24-month-old Chinese Han boy born to non-consanguineous healthy parents. Mechanically induced blistering was first noticed on his feet at the age of 6 months and then sparsely occurred on his fingers, cheek, jaw, outer ears and umbilicus (Fig. 1a). Blisters and erosions healed well without scarring, milia or atrophy. Nail dystrophy affecting all fingernails and toenails was documented (Fig. 1b). No enamel hypoplasia or dental caries were observed. Three onsets of corneal erosions following minor friction were documented at 3 month, 8 months and 1 year of age. Dysuria was present in the first year of life. By the age of 20 months, his urinary manifestation had progressively worsened with presentation of macrohaematuria and painful urination. Ultrasound examination showed left vesicoureteral reflux. Voiding cystourethrography showed bladder spasm, as well as dilatation of the posterior urethra and urethral bulb, indicating a probable anterior urethra stenosis. Magnetic resonance urography revealed bilateral ureteral stenosis, hydronephrosis, hydroureterosis, ureterectasia, and thickened bladder wall. To avoid iatrogenic injuries or blistering, instrumentation or other surgical intervention was not performed; the boy was able to urinate anyway.
This study was approved by the Clinical Research Ethics Committee of Peking University First Hospital in accordance to principles of the Declarations of Helsinki. After obtaining the informed consent from the parents, blood was obtained from the patient and his parents and a biopsy was taken from the blistered skin of the patient. Genomic DNA was extracted from the peripheral blood.
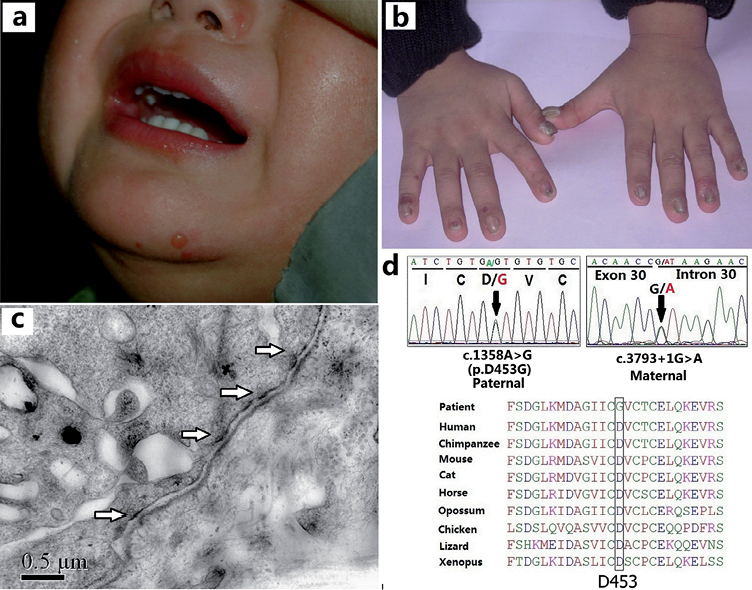
Fig. 1. Mild blistering formation in the patient at the age of 24 months (a). Nail dystrophy and thickening affecting all fingernails (b). Transmission electron microscope examination of the lesion skin showed that the hemidesmosomes (arrows) were rudimentary and reduced in number (c). Identification of compound heterozygous mutations (c.1358A>G/c.3793+1G>A) in ITGB4 and the conservation among species of amino acid position D453 (below) (d).
On a follow-up visit at 40 months of age, no blistering had occurred for 6 months. In contrast, onychodystrophy as well as symptoms of urinary tract obstruction persisted. As a result, the patient had developed rectal prolapse due to constant and excessive effort when urination. There was no growth or mental retardation. No gastrointestinal stenosis or atresia or any signs of digestive tract obstruction was documented.
Transmission electron microscope examination demonstrated hypoplastic, reduced hemidesmosomes (HDs) (Fig. 1c), which were the hallmarks of JEB.
Mutation screening of ITGB4 gene revealed that the patient was compound heterozygous for the paternal mutation c.1358A>G (p.D453G) in exon 11 and the maternal mutation c.3793+1G>A (Fig. 1d). The former mutation was novel and not found in 200 unrelated Chinese controls, whereas the latter one has previously been reported in JEB-PA, which caused aberrant splicing in the patient (5, 6). By PolyPhen-2 algorithm, the novel p.D453G mutation is predicted to be “probably damaging” with a score of 0.994. The affected D453 residue is highly conserved among species (Fig. 1d). No pathogenic mutations were found in ITGA6 or laminin-332 genes.
DISCUSSION
Of only 8 ITGB4-associated JEB cases without PA reported to date (3, 4, 7–9), 2 had generalised blistering tendency (4, 9), while other 6 had localised and mild skin involvement (3, 7–9). Notably, our patient presented with very mild blistering since birth and his skin was free of blistering after the age of 34 months. Although blistering tends to improve with age through splicing modulation in a few JEB-PA cases (7), such an early complete amelioration is uncommon. Further follow-up on this patient is ongoing.
Urinary tract complications, including urethral stenosis (dysuria, rectal prolapse) and ureteral stenosis (hydronephrosis, ureterectasia), became a major problem which persisted in our patient. This is consistent with a recent study by Schumann et al. (3) where 5 of 8 ITGB4-associated JEB patients had urinary tract involvement. A previous large-scale review also indicated that JEB more often associated with urologic complications than other subtypes (2).
Integrin α6β4 functions as a transmembrane receptor that is predominantly expressed in skin, gastrointestinal and urinary epithelia (3, 7). This non-covalent adhesive heterodimer, together with plectin and laminin-332, provides the integrity and stability to the HD anchoring complex (10). Genetic mutations in β4 subunits, which disrupt its interaction with the HD protein components, may result in HD disassembly. The p.D453G mutation found in our patient is located at the integrin β4 extracellular domain which is critical for laminin-332 binding (10). The paternal splicing mutation, c.3793+1G>A, has been shown to create 2 cryptic splice sites, both leading to a downstream premature termination codon which results in the truncated β4 subunit (5). In previous studies, homozygous c.3793+1G>A led to a lethal phenotype with PA (5), while a patient compound heterozygous for c.3793+1G>A and p.W1478X had good overall skin condition but recurrent dysuria, and congenital PA (6). The reason why p.D453G detected in our patient has a rescue effect on his gastrointestinal but not on his urinary system remains to be elucidated.
ACKNOWLEDGEMENTS
We thank the family who participated in this study. We also thank Dr. Hui Guo at Tsinghua University First Hospital for his assistance of follow-up on our patient. This work was supported by National Natural Science Foundation of China (Grant No. 81271744 & 81201220).
References

