


Zhiliang Li, Jiechen Zhang, Haoxiang Xu, Peiying Jin, Suying Feng and Baoxi Wang
Jiangsu Key Laboratory of Molecular Biology for Skin Diseases and STIs, Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing, China
Pemphigus is an autoimmune disease characterised by anti-desmoglein (Dsg) antibodies in the serum of patients. The disease can be divided into pemphigus foliaceus and pemphigus vulgaris. Anti-Dsg1 antibody is generally related to pemphigus with cutaneous lesion, and the anti-Dsg3 antibody is related to pemphigus with mucosa lesion. Twenty-nine patients with pemphigus vulgaris were selected in the clinical study. The severity of the cutaneous and mucosa lesions of these patients was evaluated using Pemphigus disease area index (PDAI). Conventional and conformational anti-Dsg index values were determined using enzyme-linked immunosorbent assay (ELISA) and ethylenediaminetetraacetic acid-treated ELISA, respectively. The relationship between clinical phenotypes and immunological profiles was analysed. In the correlation analysis, both the conventional and conformational anti-Dsg1 ELISA index values were correlated with the total and cutaneous PDAIs. In addition, conformational anti-Dsg3 ELISA index values exhibited a positive correlation with cutaneous PDAI in both types of pemphigus vulgaris, whereas no correlation was observed for the conventional anti-Dsg3 ELISA index values. Key words: EDTA-treated ELISA; pemphigus disease area index; desmoglein; pemphigus vulgaris.
Accepted Sep 1, 2014; Epub ahead of print Sep 2, 2014
Acta Derm Venereol
Suying Feng and Baoxi Wang, Jiangsu Key Laboratory of Molecular Biology for Skin Diseases and STIs, Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College Jiangwangmiao Street 12, Nanjing, Jiangsu 210042, China. E-mails: fengsy@pumcderm.cams.cn and wangbx@ncstdlc.org
The detection of desmoglein (Dsg) antibodies in the serum of patients is important in the diagnosis of pemphigus. Previous research confirmed the positive correlations between anti-Dsg1 autoantibodies and activities of cutaneous lesions (1). However, the relation between anti-Dsg3 autoantibodies and disease activity is controversial (2, 3). Conventional enzyme-linked immunosorbent assay (ELISA) detected antibodies targeted all antigen epitopes of Dsg. These epitopes include the pathogenic and non-pathogenic epitopes. Kamiya et al. (4) combined ethylenediaminetetraacetic acid (EDTA)-treated ELISA and conventional ELISA to detect the antibodies against the calcium-dependent conformational epitope, which is also referred to as the pathogenic antibodies. They found that the conformational Dsg3 ELISA index values correlated with disease activity, and they especially focused on the low Pemphigus Disease area index (PDAI) scores (5). We collected 54 serum samples from 29 patients with pemphigus vulgaris (PV) and assessed the correlation of Dsg antibodies and pemphigus subtypes. Moreover, the relationship between the ELISA index values of pemphigus autoantibodies (both conventional and conformational) and total or location-dependent PDAI scores was analysed.
MATERIAL AND METHODS
Patients with pemphigus vulgaris
Twenty-nine patients with PV were enrolled in the study from December 2011 to February 2014 (Table SI1). For all patients, diagnosis was confirmed by history (suprabasal cleft and acantholysis in biopsy specimen), direct and indirect immunofluorescence, as well as by the detection of circulating anti-Dsg1 or anti-Dsg3 autoantibodies. After obtaining written informed consent from patients, serum samples were collected and stored at –70°C. A total of 54 serum samples from the 29 PV patients were analysed. Multiple samples (2–3) from 17 patients were collected over a period of one month to 3 months.
Disease activity
The PDAI score is the main index of disease activity (6). The clinical case was evaluated using the total and location-dependent PDAI scores. Location-dependent scores include the PDAI scores for cutaneous and membrane lesions. The PDAI score for cutaneous lesions was defined as the sum of PDAI-skin score and PDAI-scalp score. Both PDAI-skin and PDAI-scalp scores were defined as the sum of activity and damage scores. All scores were measured by one specific dermatologist of the research group to avoid measurement bias.
EDTA-treated ELISA and conformational ELISA index value
Immunoreactivity was evaluated using the Dsg ELISA according to the kit manufacturer’s instructions (MBL, Nagoya, Japan). In order to modify the Ca2+-dependent epitopes of Dsg1 and Dsg3 molecules coated on the ELISA plate, the plates were treated with 0.5 mmol l–1 EDTA for 30 min at room temperature. After washing 4 times with Dsg ELISA wash buffer, the conventional assay protocol was carried out. Both EDTA-untreated and EDTA-treated ELISAs were performed with the same samples at the same time. The differences between EDTA-untreated and EDTA-treated ELISA index values were calculated as conformational ELISA index values (4). Highly reactive patients’ sera, with index values higher than 150 U/ml, were serially diluted up to 1/1600 (7).
Statistical analysis
Data analysis was performed using the Statistical Package for Social Sciences (SPSS 19.0). All tests were two-sided, and the significance level was set at p = 0.05. The Mann–Whitney U-test was used to compare the differences between conventional and conformational ELISA index values. Spearman’s rank correlation coefficient was used in statistical analysis to determine the correlation between ELISA index values and PDAI scores.
RESULTS
Anti-Dsg profile and phenotypes
Twenty-nine PV patients were divided into 2 subtypes. Mucocutaneous was the more frequent phenotype and was observed in 21 cases (72.4%). Cutaneous dominant phenotypes were observed in 8 (27.6%) cases, and histological examination of the cutaneous lesions demonstrated suprabasilar acantholysis. Among the 21 mucocutaneous PV patients, solely positive anti-Dsg1 or anti-Dsg3 was observed in 2 patients. Anti-Dsg1 antibodies were detected in 8 patients with cutaneous dominant phenotype, whereas anti-Dsg3 antibody was detected in 7 patients (Table I).
Table I. The frequency of positive anti-Dsg1 and anti-Dsg3 in different pemphigus vulgaris phenotypes
|
Mucocutaneous (n = 21) n (%) |
Cutanous (n = 8) n (%) |
Total (n = 29) n (%) |
|
|
Anti-Dsg1+ |
19 (90.5) |
8 (100) |
27 (93.1) |
|
Anti-Dsg3+ |
19 (90.5) |
7 (87.5) |
26 (89.7) |
Correlation of anti-Dsg1 index value with PDAI
The anti-Dsg1 antibody index values detected by EDTA-treated ELISA were very low. Consequently, the conformational ELISA index values of anti-Dsg1 calculated by EDTA-treated ELISA and conventional ELISA were similar to those of the conventional ELISA index values in most patients (Fig. 1). Both conventional and conformational anti-Dsg1 ELISA index values were correlated to the total PDAI (Spearman rank correlation of 0.579 and 0.547, p < 0.001) and cutaneous PDAI (Spearman rank correlation of 0.715 and 0.685, p < 0.001), but were unrelated to the mucosal PDAI (Spearman rank correlation of 0.102 and 0.087, p = 0.462 and 0.534, respectively) (Table II).
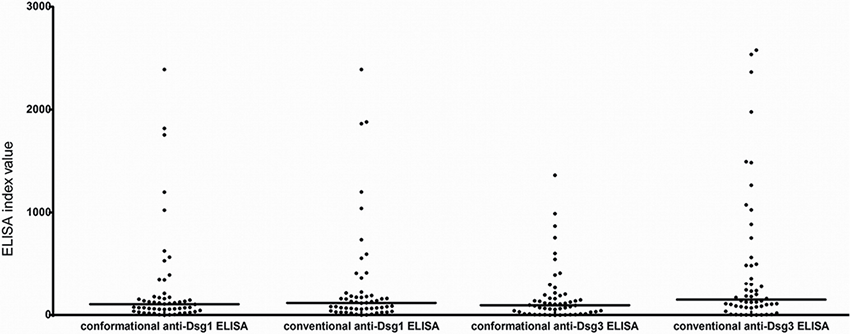
Fig. 1. Scatter plot representation of ELISA index values. Conventional anti-Dsg1 ELISA index values were similar to conformational ELISA index values (p = 0.489). However, conventional anti-Dsg3 ELISA index values were significantly higher than conformational ELISA index values (p = 0.02). Bars indicate median values.
Correlation of anti-Dsg3 index value with PDAI
Unlike the case of the anti-Dsg1 ELISA index values, several patients showed a significant gap between the conventional and conformational anti-Dsg3 ELISA index values (Fig. 1). High titres of conventional anti-Dsg3 antibodies were still detected in some patients during remission, whereas conformational ELISA index values were low (for example, cases 23, 24 and 29; Fig. 2). Both conventional and conformational anti-Dsg3 ELISA index values exhibited positive correlations with the total and mucosal PDAI, whereas conformational ELISA index values showed a better correlation (Spearman rank correlation, 0.529 and 0.383, respectively, p < 0.001 and p = 0.004, respectively). Conventional anti-Dsg3 ELISA index values showed no correlation with the cutaneous PDAI scores in both mucocutaneous and cutaneous PV patients. However, positive correlation was observed between the conformational anti-Dsg3 ELISA index values and cutaneous PDAI in PV (p = 0.002) and its subtypes (p = 0.016 in mucocutaneous PV and p = 0.027 in cutaneous PV) (Table II).
Table II. Rh- and p-values of conventional and conformational ELISA index values and Pemphigus Disease Area Index (PDAI) scores
|
Phenotype |
PDAI |
Conventional anti-Dsg1 |
Conformational anti-Dsg1 |
Conventional anti-Dsg3 |
Conformational anti-Dsg3 |
|
Pemphigus vulgaris (PV) (n = 54)a |
PDAI (Total) |
0.579/< 0.001 |
0.547/< 0.001 |
0.365/0.007 |
0.529/< 0.001 |
|
Cutaneous lesions score |
0.715/< 0.001 |
0.685/< 0.001 |
0.236/0.086 |
0.404/0.002 |
|
|
Mucous membranes score |
0.102/0.462 |
0.087/0.534 |
0.288/0.035 |
0.383/0.004 |
|
|
Mucocutaneous PV (n = 40)a |
PDAI, total |
0.518/0.001 |
0.477/0.002 |
0.312/0.050 |
0.499/0.001 |
|
Cutaneous lesions score |
0.656/< 0.001 |
0.621/< 0.001 |
0.166/0.307 |
0.377/0.016 |
|
|
Mucous membranes score |
0.255/0.112 |
0.237/0.142 |
0.358/0.024 |
0.463/0.003 |
|
|
Cutaneous PV (n = 14)a |
PDAI, total |
0.884/< 0.001 |
0.884/< 0.001 |
0.469/0.09 |
0.589/0.027 |
|
Cutaneous lesions score |
0.884/< 0.001 |
0.884/< 0.001 |
0.469/0.09 |
0.589/0.027 |
|
|
Mucous membranes score |
– |
– |
– |
– |
an referes to the number of serum samples from a total of 29 patients.
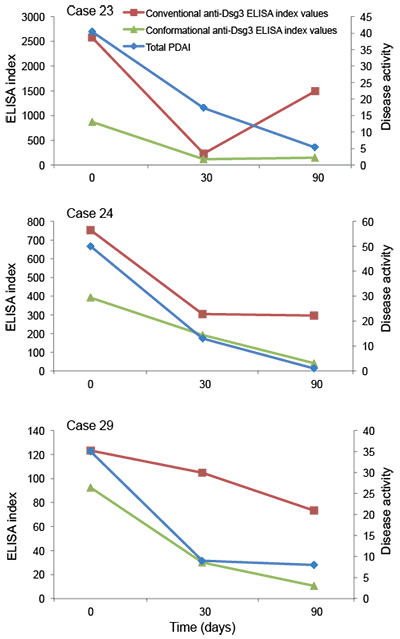
Fig. 2. ELISA index values and total PDAI scores (Disease activity) in clinical course of 3 pemphigus vulgaris patients. Conventional anti-Dsg3 ELISA index values were still high in remission; however, conformational ELISA index values were significantly low.
DISCUSSION
This research included 29 PV patients, who were divided into mucocutaneous and cutaneous phenotype groups. The mucosal dominant phenotypes were not collected probably because our institution is a dermatology-specialised hospital. Thus, patients with mucosal dominant pemphigus proceeded to a dental clinic.
In 2 of the mucocutaneous PV patients, only anti-Dsg1 antibody was detected in the serum, and no anti-Dsg3 antibody was found. This result does not conform to the “Dsg compensation theory.” Koga et al. (8) also reported 3 mucocutaneous PV cases with only the anti-Dsg1 antibody. The reason why mucosa lesions development in anti-Dsg3-negative patients include: mucosa lesions can be induced by several kinds of anti-Dsg1 antibodies that can also induce mucosa injury; other autoantibodies against keratinocytes, such as antibodies against acetylcholine receptor (9), desmocollin (10, 11), and plakoglobin (12), may be present in the patient serum. We also found 8 PV patients with solely cutaneous lesions, which is rare in clinical practice. Cutaneous type pemphigus without mucosal involvement was also reported by Yoshida et al. (13), who detected anti-Dsg3 antibodies in all their reported patients. Patients with anti-Dsg3 antibody did not develop mucosal lesions probably because of the higher Dsg3 expression in the oral mucosa. However, the anti-Dsg3 autoantibody was not adequately potent to induce acantholysis in mucosa. Furthermore, the cutaneous dominant PV may be a transient phenotype that can develop from or evolve into the mucocutaneous phenotype.
A previous study has revealed that antibodies against the Dsg conformational epitope are pathogenic. Most conformational epitopes are located on the extracellular EC1 and EC2 domains of Dsg, and such epitopes are calcium-dependent. In the ELISA experiment, the conformational epitope can be destroyed after treatment with EDTA. The ELISA index value of antibodies against the non-conformational epitope can be detected using this method. Therefore, the conformational ELISA index value can be determined by subtracting the EDTA-treated ELISA index values from the conventional ELISA index values. In this study, the conformational ELISA index values of anti-Dsg1 were similar to those of conventional ELISA index values in most patients, indicating that most portions of the anti-Dsg1 antibodies in the serum of patients target the pathogenic conformational epitope. This result agrees with that of Ohyama et al. (14), who used domain-swap technology.
A significant gap between the conventional and conformational anti-Dsg3 ELISA index values were found in the serum of several patients. This result indicated that non-pathogenic antibodies were present in the serum of these patients and that the conventional ELISA index did not reflect the changes in disease activity, which is consistent with the findings of Kamiya et al. (4) and Patsatsi et al. (1). In the correlation analysis, the titres of conformational anti-Dsg3 ELISA index values were not only found to be related to the activities of mucosal lesions, but also to the activities of cutaneous lesions. Daneshpazhooh et al. (3) used another scoring system to assess the disease severity of PV patients and found a weak correlation between the conventional anti-Dsg3 ELISA index values and the severity of skin involvement. Patsatsi et al. (1) found no significant correlation between the conventional anti-Dsg3 ELISA index values and any of the clinical scores, including the autoimmune bullous skin disorder intensity score and the PDAI scoring system. This study is the first to demonstrate a positive correlation between anti-Dsg3 ELISA index values and activities of cutaneous lesions detected by PDAI in PV patients.
In conclusion, conventional and conformational anti-Dsg1 ELISA index values can equally reflect the disease activity in PV patients, therefore, EDTA-treated ELISA is not needed in clinical work. Conventional anti-Dsg3 ELISA index values cannot reflect the disease activity in some PV patients, whereas conformational ELISA index values can rule out the non-pathogenic anti-Dsg3 antibodies, thus showing the correlations with both total and cutaneous PDAIs in PV patients. Therefore, conformational ELISA can be used as a reliable indicator in reflecting disease activities in PV patients.
ACKNOWLEDGEMENTS
The study was supported in part by The Research Special Fund for Public Welfare Industry of Health: Guideline-oriented Research in the Management of Some Common and Severe Skin Diseases (201002016).

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1961
REFERENCES


