


Masataka Tokuzumi1, Tomomi Fujisawa1, En Shu1, Hiroyuki Kanoh1, Chiemi Saigo2, Tatsuhiko Miyazaki2, Yasuhito Hamaguchi3 and Mariko Seishima1*
1Department of Dermatology, Gifu University Graduate School of Medicine, 1-1 Yanagido, Gifu, 501-1194, 2Division of Pathology, Gifu University Hospital, Gifu and 3Department of Dermatology, Faculty of Medicine, Institute of Medical, Pharmaceutical and Health Sciences, Kanazawa University, Kanazawa, Japan. *E-mail: marikoseishima@yahoo.co.jp
Accepted Oct 16, 2014; Epub ahead of print Oct 17, 2014
The signal recognition particle (SRP), an intracytoplasmic ribonucleoprotein complex of 6 polypeptides and a single 7SL RNA molecule, binds to the SRP receptor on the endoplasmic reticulum (1). Anti-SRP antibody is associated with a type of necrotising myopathy characterised by severe progressive proximal muscle weakness and high serum creatine kinase (CK) levels (1–3). It has been shown that anti-SRP antibody titres are correlated with the serum CK levels, and that plasmapheresis improves the muscle symptoms by reducing the antibody titres (4). These findings suggest that the anti-SRP antibodies may be involved in the pathogenesis of the myopathy; however, the mechanism remains unclear (5, 6). Although muscle weakness without skin eruption is considered a characteristic clinical feature of anti-SRP antibody-positive myopathy, there are a few patients with dermatomyositis (DM)-like skin eruptions and patients without muscle symptoms (6). While the disease is subacute in most cases, it can also be chronic (7). We present here a patient with anti-SRP antibody-positive myopathy, universal alopecia, and multiple vitiligo lesions without muscle symptoms.
Case report
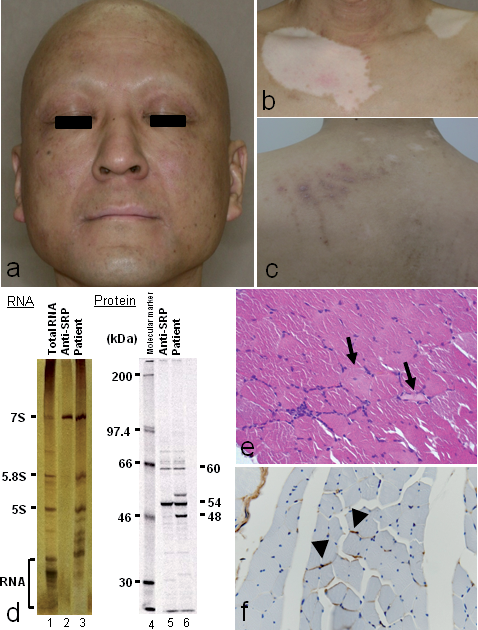
A 49-year-old Japanese man with a 12-year history of universal alopecia and a 5-year history of multiple vitiligo lesions visited our hospital because of a high serum CK level detected at a medical checkup. He had been treated for mild atopic dermatitis with topical steroids and oral administration of antihistamines since he was 20 years old. He did not complain of muscle pain, muscle weakness, itchiness, dry mouth, or dry eyes. Physical examination revealed universal alopecia, including the scalp, eyelashes, eyebrows, axillary hair, and pubic hair (Fig. 1a), and multiple vitiligo on the neck, breast, back and extremities (Fig. 1b). Erythema was not observed anywhere on the skin at the time. Neurological examination did not show any abnormalities. The patient did not complain of muscle weakness and manual muscle test was normal. Magnetic resonance imaging (MRI) showed no obvious findings of myositis in either thigh.
Laboratory examination showed high serum levels of CK (2,359 IU/l; normal, 40–200), aldolase (25.8 U/l, normal, 2.1–6.1), myoglobin (1,212 ng/ml; normal, <110), and IgG (2,383 mg/dl; normal, 890–1,850). Antinuclear antibody titre was 1:80; cytoplasmic 1:40, nucleolar 1:40, and speckled 1:80. Anti-SS-A/Ro and SS-B/La antibodies, measured by ELISA were >500 U/ml and 190 U/ml, respectively. Anti-SRP antibody was detected by immunoprecipitation (Fig. 1d). Other data were within normal ranges including T3, T4, thyroid-stimulating hormone (TSH), KL-6, glucose, calcium, and cortisol. Anti-thyroid peroxidase and anti-thyroglobulin antibodies were negative. Histological findings of the biopsy specimen from the deltoid muscle showed degeneration of muscle fibres and slight endomysial lymphocytic infiltration (Fig. 1e). Immunohistochemistry using anti-C3 antibody showed C3 deposition on the surface of the muscle cells (Fig. 1f). The results of Schirmer’s test were 8 mm and 4 mm in the right and left eyes, respectively, (normal ≥ 10 mm), and the result of the Saxon test was 1.1 g/2 min of saliva (normal > 2 g/2 min). Ophthalmological findings showed partial defects of the ectocornea in both eyes using the positive fluorescein test. These results indicated oligoptyalism and reduced lacrimation, resulting in a diagnosis of Sjögren’s syndrome. The serum levels of CK, aldolase, and myoglobin gradually increased to 3,553 IU/l, 43.6 U/l, and 1,734 ng/ml, respectively, and he complained of erythema with itching on the upper back (Fig. 1c) 6 weeks after the consultation, but he did not notice muscle symptoms. A diagnosis of anti-SRP antibody-positive myopathy with Sjögren’s syndrome, universal alopecia and multiple vitiligo lesions was made. After prednisolone was given at 60 mg/day, itchy erythema rapidly resolved and the elevated CK level decreased to the basal level. The prednisolone dose was gradually reduced to 10 mg/day following the normalisation of the CK levels. However, the alopecia and vitiligo were not improved.
Discussion
We present here a patient with anti-SRP antibody positive-myopathy showing high serum CK, aldolase, and myoglobin levels in the absence of muscle weakness or muscle pain, which is uncommon. However, an asymptomatic patient with anti-SRP antibody-positive myopathy has already been reported (8). Itchy erythema, which is often observed in DM, appeared on the back at the same time as the increased serum CK level but could also be a manifestation of atopic dermatitis. Skin eruption does not typically occur with anti-SRP antibody-positive myopathy; however, a few patients have shown DM-like skin eruptions (6, 9) or finger swelling (9). The laboratory test performed 5 years previously showed antinuclear antibody 1:40 with a nucleolar and speckled pattern. The anti SS-A/Ro and SS-B/La antibodies at that time were > 500 U/ml and 142 U/ml, respectively. The cytoplasmic autoantibody pattern (anti-SRP)obviously appeared later on.
The patient also had Sjögren’s syndrome, alopecia and vilitigo. It is not uncommon that patients with anti-SRP antibody-positive myopathy have SSA/Ro antibodies and sicca symptoms (2, 6). Vitiligo is found in 4% of patients with alopecia totalis and/or universalis (11), but has not been reported in association with Sjögren’s syndrome and anti-SRP antibody-positive myopathy.
Histological examination showed muscle fibre degeneration and C3 deposition on the muscle cell surface with slight endomysial lymphocytic infiltration in the present case (Fig. 1e, 1f). These results might indicate antibody-dependent, complement-mediated muscle cell lysis (1, 5).
Patients with anti-SRP antibody-positive myopathy reportedly respond poorly to corticosteroids (4, 7); however, prednisolone rapidly resolved the high serum levels of CK, aldolase, and myoglobin in the present case. Relatively good neurological outcomes were obtained in 45% of the subacute form of anti-SRP antibody-positive myopathy (7). In addition, the responses to treatment (6) and survival rates (2) in patients with anti-SRP antibody-positive myopathy did not differ significantly from polymyositis patients without anti-SRP antibodies. Early detection of anti-SRP antibodies is important for choosing the best treatments. Because anti-SRP antibody titres are correlated with the serum CK levels, the titres could be valuable for monitoring the disease activity (4, 10). However, as quantitative tests for anti-SRP antibody titres are still not commonly available, we could not measure the titres. Further studies are required to elucidate the pathogenesis of the myopathy, including the role of the anti-SRP antibodies.
References

