


Gwennaëlle Colaianni1 and Françoise Poot2
1Department of Psychology, UCL, Louvain La Neuve, and 2Department of Dermatology, ULB-Erasme Hospital, Brussels, Belgium
Alopecia areata (patchy hairloss) often indicates to the dermatologist the existence of psychological disorders, mostly anxiety and depression. Psychosomatic conditions are usually associated with difficulty in expressing emotions, what is called alexithymia, and this difficulty is often seen in patients with alopecia areata. This case study aims to show how to help these patients connect with their emotions and how the somatic symptom can become meaningful by using a unifying approach, which challenges the beliefs, the rules and the interactions of both the individual and the family, as well as the emotions expressed or suppressed. In this particular case we used a systemic family therapy tool, “the Family Blazon” that helped to discover the unconscious myth of unity and the fear of family disaggregation that is involved in psychosomatic families. Key words: psychodermatology; psychosomatics; alopecia areata; family therapy; emotions; alexithymia; metaphoric tool.
Accepted Feb 16, 2016; Epub ahead of print Jun 9, 2016
Acta Derm Venereol 2016; Suppl 217: 109–112.
Françoise Poot, Department of Dermatology, ULB-Erasme Hospital, route de Lennik 808, BE-1070 Brussels, Belgium. E-mail: frpoot@gmail.com
All health care professionals should take an interest in the complexity of the mind–body relationship. Psychosomatic disorders offer the opportunity of understanding some of the interactions between the psyche and the soma. However, psychosomatic patients rarely go to psychologists. Instead, the problem or difficulty is expressed through body language. The difficulty these patients have in identifying and verbalizing their emotions, feelings and fantasies is called alexithymia (1). It is therefore difficult to refer these patients to a mental health professional, and furthermore some of these professionals are not well experienced in treating this type of problem. This case illustrates the necessity of reinstating the symptom into a context and viewing it as a complex, multi-determined phenomenon. It also illustrates how a specific approach, the use of a non-verbal tool, can help to connect with the underlying emotions. According to the systemic family theory, families with past traumatic experiences who show psychosomatic symptoms, appear to be stuck in rigid states where individuality is impossible due to the unconscious myth of unity and fear of disaggregation of the family. So, family members experience the conflict of being disloyal to their family if they express any wish of autonomy (2).
CASE REPORT
Raphael (invented name) is a 17-year-old boy suffering from alopecia areata from the age of 11, with instances of partial recovery and a period of alopecia totalis when he was 12. At present he has some level of patchy hair loss.
While conducting a study on psychosomatic disorders, the psychologist in our team interviewed Raphael. It was difficult to arrange an appointment for Raphael to come to the clinic, as messages were not being passed to him. They failed to keep the appointment and when they finally came, Raphael’s father indicated that they had little available time to spend in the consultation. This indicates that the family was apprehensive about their son being assessed. While answering questions, Raphael wanted his mother by his side. Together, they gave the appearance of being a couple, leaving the father as the outsider in this mother and son relationship.
Raphael is the youngest of 3 siblings. Raphael and his family have been to numerous physicians and therapists in hopes of “getting rid” of what they call “Raphael’s problem”. At our clinic, the dermatologist – who is also a family therapist – prescribed topical immunotherapy with diphenylcyclopropenone (DPCP) (3) and started a family therapy approach. Concerning the family’s history, we learned that Raphael’s birth was difficult and probably quite a traumatic event, the birth process taking over 14 h. During his early childhood, Raphael’s maternal grandfather died. The family tried to hide the body from Raphael but the boy managed to see it. This, according to his mother, was another traumatic event in her son’s life. Going to high school was reportedly another difficult experience. Currently Raphael has facial hair growth, but he shaves his head, as the hair there is not growing uniformly. He is currently a senior at high school and is faced with a decision on what to do next year. Raphael thinks that he would like to live on his own but this has not yet been discussed within the family.
Raphael’s sister worked abroad for a while but returned back home to Belgium because she missed her family. She is going to move into a house near her parents’ that belongs to her grandparents. Raphael’s brother is at university but comes home every weekend. It is very difficult for the children to move away from the family circle. Raphael’s mother is a teacher, and she is very involved with the lives of her children, especially with Raphael. According to Raphael and his mother, the father is never available, always working long hours.
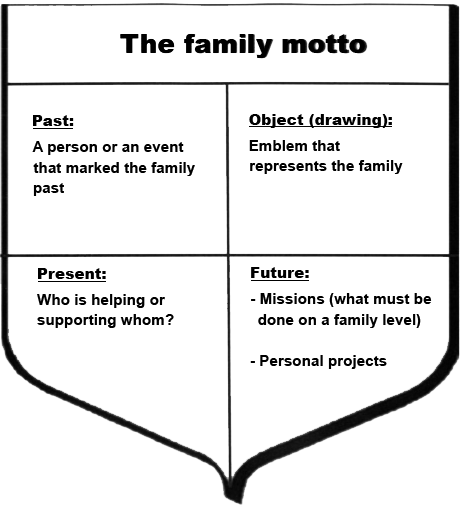
The Family Blazon (Fig. 1) is a family therapy tool used to understand the family’s present situation and their past history. It also helps to describe the family’s emotions associated to those events and how the family members see themselves. With the use of this technique the family’s timeline is recreated, including past, present and future events, as well as the “mythical” events. According to Rey (4) this is a way to think about emotion within a systemic-constructivist framework in frozen situations. The Family Blazon (Fig. 1) is divided into 4 quarters plus a space at the top for the family motto. The 4 quarters are used to record the following: the past (a person or an event that marked the family’s past), the present (alliances: which members help each other and which members are close to each other, etc.), the future (family aspirations and personal projects), and an emblem that represents the family.
Description of the Family Blazon of Raphaël’s family (Fig. 2)
Raphael and his parents express similar beliefs about the family; unity is a predominant value. Both Raphael and his mother choose the same motto when asked to express a motto that defines their family. This seems to indicate that the members of this family share an idealistic point of view concerning their family identity. This would confirm the family’s “myth” of unity.

Fig. 2. Raphael’s Family Blazon.
In the square called “the past”, the members are asked to write about a person or an event that was of significance at some time in the family’s past. Raphael and his father identify Raphael’s grandfather’s death as the most important event in family past. Raphael emphasizes the fact that he lost an important person in his life. Surprisingly, Raphael’s mother does not mention the death of her father on the blazon. Instead, she writes down: “the alopecia of our “fifi”. We learned during the interview that Raphael’s mother got along very well with her father but never could really have a discussion with her own mother. The death of her father must have been a difficult experience for her as she lost a confidant. That is why the information collected here about the past is very puzzling. Why does not she say anything about her father’s death when other family members agree that it was the most important event in the family life? Is it interesting to see how “Raphael’s problem”, the alopecia, allows the mother to focus on something other than the death of her own father. In the quarter called The Present, the members are asked about who is helping or supporting whom. All of them talked about the cohesiveness of the family.
They deny any differences, preferences and conflicts. They seem to tell us that there are no flaws in their family support. Raphael reveals an important detail. We found out that the support does not exist with other relatives other than the 5 family members. During the whole interview, Raphael’s mother draws our attention to the fact that there are “no problems” in her family. However, Raphael’s father did not fill in the square related to an object symbolizing the family, though he mentioned something about it during the interview. When we asked him how he could describe the family, Raphael’s father said: “like a block”. This is a very strong symbol that illustrates the extreme cohesiveness between family members. Just like her husband, the object chosen by Raphael’s mother contributes to reinforce the family myth of unity: an egg or a nest. Those images illustrate the deep cohesiveness, the little differentiation between members and the overprotectiveness that might probably be found in the family. As far as Raphael is concerned, he chooses a diamond because it has several facets (good and bad) and, as he told us, because the family is very precious to him. It is worthy of mention that all those objects symbolize a closed, strong and rigid system. In the portion of the blazon that represents the future, the members were asked to write about their personal projects and their family missions. This section shows a lack of interest in change and in individual evolution. Raphael’s mother does not write anything concerning her personal projects. She is focused on her maternal mission. This raises a new question: how will she face to the future when her children will not need her any longer? “Raphael’s problem”, as they call it, might allow her to keep her function in the system forever. As long as he does not totally recover, his mother will have an important role to play in the system. Raphael’s father does not mention any personal project either. He only talks about the decision that Raphael has to make to choose a college. Raphael formulates two “wishes”. The first one is personal. He wishes to be happy and to cope with his problem as well as possible. What surprises us is that he seems to have accepted the disorder in his life and is not expecting a total recovery. The second wish is to keep in touch with his sister and brother unlike what his parents have done with their siblings. Raphael tells us here that they have few contacts with their relatives. We can feel Raphael’s fear of losing touch with his own siblings. This would break the family unity.
Comments on Raphael’s Family Blazon: together with the information gathered during the interview they demonstrate a strong myth of unity that seems to govern the family. The “family picture” drawn especially by Raphael and his mother is the picture of a “happy family”, cohesive, not acknowledging any family problems. Their system of beliefs is rigidly dominated by the theme of unity. We can make two hypotheses about this: that the growing distance between the parents and their families led Raphael to fear the disaggregation of their family unity. The rule became to stay together forever, to avoid any conflicts, to suppress preferences and differences between members. We also think that the death of Raphael’s maternal grandfather played a particular role in the construction of the myth. That dramatic event happened more than 10 years ago but is still very present in everybody’s mind. At that time, Raphael’s mother lost a very important person in her life, probably the only real “bond” with her family history. And it was the beginning of Raphael’s hair loss.
The way the family history has been told by the 3 members interviewed reinforces the myth of unity. For example, special relationships between two members are constantly denied. Raphael’s mother avoids talking about her mother with whom she never got along. Moreover, Raphael’s father who only takes part in the interview a few minutes is the first one to tell us that Raphael’s mother tries to be better than her own mother with the children. We are interested in the fact that the family seems to give certain roles and functions in harmony with the transmission of the myth of unity to Raphael and his mother. Unlike Raphael’s father, they both try not to share with us any problems, any conflicts that could break the myth. Our first impression of a “happy family” is progressively replaced by a feeling that something is hidden from us, something we are not allowed to find out.
About the therapist’s emotions
According to the works of Dessoy (5) on the concept of “contact” which is one of the communication modes in the family system, we chose to verbalize what we felt when we were in contact with the family members. With psychosomatic patients who do not express their feelings, we find it very important to focus on our own emotions in order to understand the emotions felt by the patient. When we met Raphael and his family we had a very nice, enjoyable time. Raphael and his mother drew a picture of a happy, cohesive family without any problems. The first emotions we felt were very positive. We felt closed out from the members. We thought that no conflict or difficulties were to be found within the family as they kept insisting on it. However, after analyzing our emotions more carefully we realized that another kind of emotion was present. We felt uncomfortable because Raphael’s mother seemed not to allow us to look into family difficulties. She seemed very anxious whenever her son talked about differences between his siblings and kept denying any preferences or conflicts. We then felt more and more that we were in front of an “invisible problem”. Seeking for information to contradict the myth, we learned about Raphael’s fears to loose contact with his siblings in the future, comparing this situation with his parent’s family situation. The topic of loss is present at this level also.
DISCUSSION
On the basis of the analysis made, we were able to confirm that Raphael’s life had been dominated by the topic of loss. At the beginning, difficult circumstances around Raphael’s birth might have contributed to the start of the psychosomatic disorder. Raphael’s parents probably lived the event with the fear of losing their child. We can assume that parental emotional reactions are to be considered in the understanding of this particular disorder. The theme of loss also appeared during the death of Raphael’s grandfather. It is possible that Raphael’s problem diverted his mother’s attention from her own father’s death. We also found out that the family’s relationship with the parents’ families are quite poor. Raphael fears the same family disaggregation with his own brother and sister. Thanks to his disorder, family members stay together. We can see how Raphael’s alopecia arises in concordance with the family myth of unity. In the introduction, we mentioned metaphoric meanings in psychosomatic disorders. In this case, Raphael’s alopecia seems to indicate, metaphorically speaking, that “fear of loss” is present in the family. On the one hand, the psychosomatic disorder strengthens the family unity but on the other hand, the symptom is also an attempt to eradicate the myth. In Raphael’s case, “the problem” is impossible to hide. This peculiar symptom however, contradicts the family rules about not communicating what is going wrong in the family. Alopecia is probably one of the most visible psychosomatic disorder, and in Raphael’s case, it becomes the only problem “expressed” in the family. That might be the reason why no problem, no flaw can be detected, none except one that chooses body language: Raphael’s alopecia. Therefore, with such a visible disorder that makes him “different from others”, Raphael reinstates a degree of differentiation in the system.
As Byng-Hall (6) stated, “the danger is that a family myth may become a closed belief system that cannot integrate new information. This is particularly likely to happen if the family feels that a challenge to its beliefs threatens family survival. If the myth becomes closed, family interaction loses some of the advantages of the beneficial stability gained from the myth, and becomes rigidly unable to change contexts”.
That is why we choose to look at the problem through a family approach that considers the symptom in a context that gives it sense. Let us quote here Onnis et al. (7): “The symptom manifested by the patient is not the passive effect of the dysfunction of the interpersonal system in which it appears, but rather it takes on a communicative significance and plays an active (or retroactive) role in homeostatically maintaining the dysfunctional characteristics of the system. Thus, family dysfunction and the patient’s symptom are so closely and circularly linked that they reinforce and perpetuate each other”. Moreover, the symptom plays a “double” role in the family context that we cannot ignore. Onnis demonstrated the ambiguous position of the child or adolescent with the psychosomatic disorder in regard with the family myth. As therapists we should bear in mind that this supports both positions: the one that reinforces the myth by the cohesiveness found around the ill child and the other one according to which the symptom arises to reveal the inadequacy of the family’s rigid organization.
Systemic family therapy literature emphasizes the existence of family dysfunction in psychosomatic families. One of the co-author published a study on family dysfunction in psoriasis, atopic dermatitis and alopecia areata (8). We also saw the need to analyze the health professional’s emotions when meeting the family. This is especially important as each member contributes in reinforcing the myth and thus carefully avoids expressing their feelings. If we only focus on “what they say” about themselves, we miss an important source of information which could help us to understand the metaphoric meaning of the disorder. Moreover, we might take a position in the system that would reinforce the myth as well and thus prevent the family from looking to its necessary evolution. This is important for the dermatologist too: some information linked with deep, difficult emotions is carefully hidden. That is why analyzing the “contact” (emotions felt with the members) takes the caregivers to another “reality” which will help them in their task with psychosomatic patients. The metaphoric sense recovered when we analyzed the emotions felt when in contact with the family, contradicts the verbal message of the members. Siméon & Malvaux (9) in their work with obese patients also note the “heavy”, “oppressive” environment felt in contact with those patients. Thus the emotions felt by the caregiver could reveal the metaphoric sense of the disorder.
CONCLUSION
Some ideas regarding the therapy of psychosomatic patients and their families are illustrated with this case. First of all, we have to bear in mind that psychosomatic disorders are to be understood as presenting at a crossroad between biological, psychological and social factors. Denying the biological vulnerability or taking care of the psychological difficulties without “healing” the body makes our therapeutic intentions doomed to failure. Cooperation between physicians and psychotherapists should be enhanced. Alexithymia, characteristic in psychosomatic patients, forces us to use different techniques in order to access those emotions not expressed in the patient’s speech. In the present case we used the Family Blazon, however, the genogram (4), family sculptures (10) or other metaphoric tools are also useful with psychosomatic patients and their families. These techniques allow the family to get in contact with emotions linked to traumatic events, without threatening the family’s unity. Using the healer’s emotion, whether dermatologist or mental health professional, is also important to increase the perceptions of hidden problems. The difficulty when we meet these families is to enhance differentiation and individual development without disqualifying the love, protectiveness and unity found in the system, otherwise the family would raise resistances. The way to go further and to circumvent this difficulty is to work with the non-verbal and metaphoric images given by the family. We can then propose another a way to be loyal to the family that gives more freedom to the individual.
References

