


Stefano PIASERICO1#, Paolo GISONDI2#, Paolo AMERIO3, Giuseppe AMORUSO4, Anna CAMPANATI5, Andrea CONTI6, Clara DE SIMONE7, Giulio Gualdi8, Claudio GUARNERI9, Anna MAZZOTTA10, Maria L. MUSUMECI11 and Damiano ABENI12, for the ALPHARD Study Group
1Department of Medicine, Dermatology Unit, University of Padova, Padova, 2Department of Medicine, Section of Dermatology and Venereology, University of Verona, Verona, 3Department of Oncology and Neuroscience, Dermatologic Clinic, University G. D’Annunzio, Chieti, Dermatology Units, 4University of Catanzaro (Italy) C/O Fondazione per la Ricerca e la Cura dei Tumori ‘Tommaso Campanella’ COE, Germaneto di Catanzaro (CZ) and 5Marche Polytechinic University, Ancona, Departments of Dermatology, 6University of Modena and Reggio Emilia, Modena and 7Catholic University of the Sacred Heart, Rome, 8 Department of Dermatology,Spedali Civili Brescia, Brescia 9Department of Clinical Experimental Medicine, Section of Dermatology, University of Messina (Italy) c/o A.O.U. “G. Martino”, Messina, Departments of Dermatology, 10San Camillo-Forlanini Hospital, Rome and 11AOU Policlinico-Vittorio Emanuele, PO G. Rodolico, Catania, and 12Clinical Epidemiology Unit, IDI-IRCCS FLMM, Rome, Italy. #These two authors have equally contributed to the manuscript.
Psoriatic arthritis (PsA) is a potentially severe inflammatory condition (entheso-arthro-osteopathy), and early diagnosis is important to guide treatment choices in patients with psoriasis. The objective of this study is to further validate the PsA Screening and Evaluation (PASE) questionnaire, and to assess its field performance. Data were collected in 10 Italian centres, and the PASE was administered at baseline, after 3 days and after 3 months. The Skindex-29 was also administered. To determine the best cut-off value to identify patients with PsA we produced receiver operating characteristic (ROC) curves using the rheumatologist’s diagnosis as outcome. Of the 298 patients that were enrolled, 28% were classified as having PsA according to the CASPAR criteria, while 19% had received a diagnosis of PsA from a rheumatologist. PASE score were always significantly different in patients with or without PsA, while Skindex-29 scores never were. The internal consistency of the PASE was very good (Cronbach’s α of 0.90–0.95), the test–retest reliability was also very high (intraclass correlation coefficients 0.91–0.93), and the PASE scores showed good responsiveness to clinical change over time. The optimal cut-off identified through the ROC curves was ≥ 48 on the total PASE score, which was able to distinguish PsA from non-PsA patients with a 73.2% sensitivity and a 76.1% specificity. Our results confirm the good psychometric properties of the PASE, and indicate that it may be a useful tool for the dermatologists, both to screen for PsA and to obtain a standardized patient-reported measure to monitor and evaluate the health status of the patients with PsA. Key words: psoriasis; psoriatic arthritis; PASE; questionnaire: Italian version.
Accepted Apr 4, 2016; Epub ahead of print Jun 9, 2016
Acta Derm Venereol 2016; Suppl 217: 96–101.
Stefano Piaserico, MD, PhD, Dermatology Unit, Department of Medicine, University of Padua, Via Cesare Battisti 206, IT-35128 Padua, Italy. E-mail: stefano.piaserico@unipd.it
Psoriatic arthritis (PsA) is an inflammatory entheso-arthro-osteopathy occurring in subjects with psoriasis, which may involve both peripheral and axial osteo-articular compartment (1). PsA mostly affects patients between 30 and 50 years of age, and the highest prevalence is reported from Northern Europe. The reported prevalence of PsA in patients with psoriasis ranges from 6% to 42% according to different studies (1, 2). Dermatologists are in a strategic position for the early recognition of PsA, because in most instances skin symptoms may precede joint symptoms (3). Ideally, every psoriasis patient with musculoskeletal pain should be evaluated by a rheumatologist, but this is not really practical and cost-effective. Accordingly, screening questionnaires to be used in the dermatology or general practice setting to identify psoriatic patients who refer symptoms suggestive for PsA have been developed (4–7). These include the Toronto Psoriatic Arthritis Screen (ToPAS) screening questionnaire, the Psoriatic Arthritis Screening and Evaluation (PASE) questionnaire, the Psoriasis Epidemiology Screening Tool (PEST) questionnaire and the early PsA-screening questionnaire. The use of a validated questionnaire is a simple and fast tool for the identification of those patients who are more likely to need a rheumatologic referral because of suspicious PsA. The PASE questionnaire is a self-administered tool that can be used to screen for PsA among patients with psoriasis. PASE has proven to be able to distinguish between symptoms of PsA and osteoarthritis. The purpose of this study is to validate the PASE in the Italian language, and to investigate whether it may be used not only as a screening tool but also as an evaluative instrument to monitor the effectiveness of treatment.
Materials and methods
Population
This multicentre study was conducted in the dermatological outpatient clinics of 9 Italian universities: Three from Northern Italy, i.e., Modena, Padova and Verona; 4 from Central Italy, i.e., Ancona, Chieti, Tor Vergata in Rome, and the Catholic University also in Rome; and 3 from Southern Italy, i.e., Catania, Catanzaro, and Messina. The study was approved by the Ethical Committee of each participating centre.
The inclusion criteria were: age ≥18 years, diagnosis of plaque psoriasis according to the Italian Guidelines, ability to read and understand the Italian language, signed written informed consent. The exclusion criteria were: major psychiatric morbidity (e.g., depression, schizophrenia, bipolar disorders), previously diagnosed autoimmune disorders (e.g., ankylosing spondylitis, rheumatoid arthritis, systemic sclerosis, coeliac disease, multiple sclerosis), positivity for the rheumatoid factor confirmed by positivity for anti-citrullinated protein antibodies; present treatment since over 3 weeks with non-steroid anti-inflammatory drugs, cortison, disease-modifying antirheumatic drugs, or systemic drugs for psoriasis; presence of pustular or erythrodermic psoriasis.
Data collection
At baseline, patients who signed the informed consent were asked to complete the following questionnaires: the PASE, the Skindex-29 – from which the scores of the two scales of the Skindex-17 were also derived – and the 12-item General Health Questionnaire (GHQ-12).
The dermatologists collected socio-demographic and clinical information, scored the clinical severity at baseline according to the 7-point Physician Global Assessment (PGA), ranging from 0 (no skin involvement) to 6 (very severe involvement), and calculated the Psoriasis Area and Severity Index (PASI). They also completed the Psoriasis Epidemiology Screening Tool (PEST) (5) and recorded whether a diagnosis of PsA had already been made by a rheumatologist.
Three to 7 days after baseline the PASE was re-administrated to the same patients, in order to evaluate the test-retest reliability. After 3 months, the PASE, the Skindex-29, and the GHQ-12 were administered again. The dermatologist completed again the PASI, and recorded a general evaluation of the patients’ clinical improvement/worsening on an 8-point scale, from –3 (very much worsened) to +4 (cleared), with 0 meaning no clinical change. The same scale was used by the patients to record their impression of the clinical change.
Diagnostic criteria for psoriatic arthritis
The Classification Criteria for Psoriatic Arthritis (CASPAR) criteria for PsA consist of inflammatory articular disease (joint, spine, or entheseal) with ≥ 3 points from the above categories. The sensitivity is 98.7% and the specificity is 91.4%. Evidence of current psoriasis, a personal history of psoriasis, or a family history of psoriasis (2 points). Current psoriasis is defined as psoriatic skin or scalp disease present today as judged by a rheumatologist or dermatologist. A personal history of psoriasis is defined as a history of psoriasis that may be obtained from a patient, family physician, dermatologist, rheumatologist, or other qualified health care provider. A family history of psoriasis is defined as a history of psoriasis in a first- or second-degree relative according to patient report. Typical psoriatic nail dystrophy including onycholysis, pitting, and hyperkeratosis observed on current physical examination (1 point). A negative test result for the presence of rheumatoid factor (1 point). Either current dactylitis, defined as swelling of an entire digit, or a history of dactylitis recorded by a rheumatologist (1 point). Radiographic evidence of juxta-articular new bone formation appearing as ill-defined ossification near joint margins (but excluding osteophyte formation) on plain radiographs of the hand or foot (1 point).
PASE
The PASE questionnaire has been proposed as a self-administered tool that can be used to screen for PsA among patients with psoriasis (6, 8). In principle, it can also measure the level of impairment that PsA causes to patients. It consists of 15 items, with possible answers on 5 levels, scored from 1 to 5: “strongly disagree”, “disagree”, “neutral”, “agree”, “strongly agree”. It is subdivided into two scales: the symptoms scale includes 7 items (possible range 7 to 35), and the Function scale includes 8 items (possible range 8 to 40). The sum of the two subscales yields the total PASE score, with a possible range of 15 to 75. Higher scores indicate a higher probability of PsA, and a higher level of impairment.
To obtain a valid Italian version of the PASE, we followed the guidelines for the cross-cultural adaptation of health-related quality of life (QoL) measures (9). The first translation was produced by one of the authors (DA) and a second one was produced by another author (SP). The two versions were compared and discussed during a meeting of all authors, who agreed on a single version incorporating aspects of both preliminary translations. This version was back translated by an English mother tongue expert who was not otherwise involved with this study. The back translation was reviewed by DA and a final Italian version was created.
Skindex-29 and Skindex-17
The Skindex-29 (10, 11) is a dermatological QoL instrument which consists of 29 items, with possible answers on a 5-point scale, from “never” to “all the time”. It is constituted by 3 subscales, measuring symptoms, emotions and functioning. Higher scores indicate a higher burden on QoL.
The Skindex-17 was derived from the Skindex-29 using Rasch analysis (12, 13). It is composed of 17 items subdivided into the symptoms and the psychosocial subscales, and answers are given on a 3-point scale instead of a 5-point scale.
GHQ-12
The GHQ-12 is a self-administered questionnaire designed to measure psychological distress and to detect current nonpsychotic psychiatric disorders, such as anxiety or depression (14). It has been extensively validated in dermatological settings (15). Answers are given on a 4-point scale and scored as 0-0-1-1. A score of 4 or more indicates the possible presence of anxiety or depression.
Statistical analyses
Descriptive data were reported using percentages and means. Mean values were compared using the t-test or ANOVA. The internal consistency of the PASE was assessed by means of Cronbach’s α. The test–retest reliability was measured by the correlation between the scores at baseline and after 3–7 days, using the intraclass correlation coefficient which is equivalent to the Kappa statistic for continuous values. It has the advantage over the Pearson’s or Spearman’s correlation coefficient in that it is a true measure of agreement, combining information on both the correlation and the systematic differences between the readings (16).
Construct validity was assessed hypothesising that patients with a more severe joint involvement would score higher than patients with a mild disease.
The convergent validity was assessed by examining the correlation between the PEST and the symptoms, function, and total PASE scores. The correlations with the scales of the Skindex-29, Skindex-17, and of the GHQ-12, as well as the one with the PASI and the visual analogue scale (VAS) for pain, were also studied.
The responsiveness was studied comparing the differences of the PASE score at baseline and after 3 months in relation to the clinical change perceived by the patient. The evaluation of clinical change by the patients was grouped into 4 categories: “no or slight improvement”, “moderate improvement”, “substantial improvement”, and “healed”. The score variations were evaluated by the Wilcoxon test for dependent data.
The cut-off for the dichotomization of the PASE scores was determined using receiver operating characteristics (ROC) curve, using as an outcome the rheumatologist’s diagnosis.
All statistical analyses were performed using the statistical package IBM SPSS Statistics, version 21 (SPSS, Chicago, IL, USA).
Results
A total of 298 patients were enrolled in the study centres. The distribution of the study population for the main variables of interest is described in the first two columns of Table I. Typically for psoriasis studies, most patients were male (56.4%). Over 50% had a PASI score of ≥ 10, and 28% were classified as having PsA according to the CASPAR criteria, while 19% had received a diagnosis of PsA from a rheumatologist. Over half of the study population was either overweight (34.5%) or obese (20.7%). Also of note is the proportion of patients classified as GHQ-12 positive (35.4%), indicating that over one third of the study sample had a probable minor non-psychotic psychiatric disorder, such as a tendency to depression and anxiety.
Table I. Composition of the study population, and mean Psoriatic arthritis Screening and Evaluation (PASE) and Skindex-29 scores for all the levels of the main variables of interest
|
Variable |
n (%) |
PASE |
Skindex-29 |
|||||
|
Sym |
Func |
Tot |
Sym |
Emot |
Func |
|||
|
Overall |
298 (100) |
19.6 |
21.3 |
40.9 |
50.3 |
45.7 |
36.4 |
|
|
Gender |
||||||||
|
Female |
130 (43.6) |
20.8 |
22.2 |
43.0 |
53.1 |
49.1 |
38.1 |
|
|
Male |
168 (56.4) |
18.6 |
20.4 |
39.4 |
48.2 |
43.0 |
35.1 |
|
|
p-values |
0.007 |
0.122 |
0.032 |
0.051 |
0.026 |
0.312 |
||
|
Age, years |
||||||||
|
< 40 |
103 (35.0) |
17.3 |
18.6 |
36.0 |
50.4 |
46.3 |
33.1 |
|
|
40–59 |
106 (36.1) |
20.6 |
22.7 |
43.3 |
50.4 |
46.0 |
38.8 |
|
|
> 60 |
85 (28.9) |
21.2 |
23.2 |
44.4 |
49.9 |
44.6 |
37.8 |
|
|
p-values |
< 0.001 |
< 0.001 |
< 0.001 |
0.986 |
0.874 |
0.212 |
||
|
Body mass index |
||||||||
|
< 25 |
130 (44.8) |
18.9 |
20.2 |
39.1 |
48.3 |
44.6 |
34.7 |
|
|
25–29 |
100 (34.5) |
19.7 |
21.4 |
41.2 |
51.9 |
47.4 |
39.8 |
|
|
> 30 |
60 (20.7) |
20.7 |
23.6 |
44.3 |
51.2 |
44.1 |
34.0 |
|
|
p-values |
0.221 |
0.034 |
0.073 |
0.411 |
0.584 |
0.210 |
||
|
Psoriasis Area and Severity Index (PASI) |
||||||||
|
< 10 |
131 (45.2) |
19.8 |
21.0 |
40.8 |
46.4 |
39.6 |
29.7 |
|
|
10–14 |
67 (23.1) |
18.9 |
21.2 |
40.1 |
53.3 |
47.5 |
38.1 |
|
|
> 15 |
92 (31.7) |
19.9 |
22.0 |
41.9 |
54.0 |
53.5 |
45.2 |
|
|
p-values |
0.657 |
0.642 |
0.723 |
0.017 |
< 0.001 |
< 0.001 |
||
|
Physician Global Assessment (PGA) |
||||||||
|
Mild |
63 (21.2) |
19.6 |
21.2 |
40.8 |
43.5 |
35.5 |
22.2 |
|
|
Moderate |
134 (45.1) |
18.6 |
20.2 |
38.8 |
49.6 |
43.7 |
34.8 |
|
|
Severe |
100 (33.7) |
21.0 |
23.1 |
44.1 |
55.4 |
54.9 |
47.7 |
|
|
p-values |
0.031 |
0.028 |
0.022 |
0.003 |
< 0.001 |
< 0.001 |
||
|
PsA (Rheumatologist)a |
||||||||
|
No |
240 (81.1) |
18.2 |
19.7 |
37.9 |
49.9 |
45.3 |
35.3 |
|
|
Yes |
56 (18.9) |
25.8 |
28.9 |
54.7 |
51.8 |
47.5 |
41.7 |
|
|
p-values |
< 0.001 |
< 0.001 |
< 0.001 |
0.566 |
0.532 |
0.087 |
||
|
PsA (CASPAR)b |
||||||||
|
No |
212 (71.9) |
17.6 |
19.1 |
36.7 |
49.2 |
44.7 |
34.7 |
|
|
Yes |
83 (28.1) |
24.8 |
27.3 |
52.1 |
53.5 |
48.2 |
41.2 |
|
|
p-values |
< 0.001 |
< 0.001 |
< 0.001 |
0.130 |
0.250 |
0.045 |
||
|
12-item General Health Questionnaire (GHQ-12) |
||||||||
|
Neg. |
192 (64.6) |
17.8 |
19.2 |
37.0 |
44.1 |
37.9 |
27.6 |
|
|
Pos. |
105 (35.4) |
22.8 |
25.2 |
48.0 |
61.7 |
60.2 |
52.9 |
|
|
p-values |
< 0.001 |
< 0.001 |
< 0.001 |
< 0.001 |
< 0.001 |
< 0.001 |
||
aPresence of psoriatic arthritis (PsA) according to a diagnosis by a rheumatologist. bPresence of PsA according to the Classification Criteria for Psoriatic Arthritis.
Sym: symptoms; Func: functioning; Tot: total; Emot: emotions.
Table I also summarizes the mean scores of PASE and Skindex-29 for the different levels of the main variables of interest. First of all, construct validity seems to be supported by highly statistically significant differences in PASE scores between patients with and without both a CASPAR or a rheumatologist’s diagnosis of PsA. It is interesting to note that such difference does not appear to be significant for the generic dermatological instrument. Also, the PASE score are significantly elevated for older patients, for obese individuals, and for those classified as “severe” by the GPA. On the other hand, it is also interesting to point out that the PASE scores are only marginally affected by the PASI, while the Skindex-29 shows large, and statistically significant differences, between the different levels of PASI score.
The internal consistency of the PASE was very good, as indicated by the Cronbach’s α of 0.90 for the symptoms subscale, 0.93 for the function subscale, and 0.95 for the total score. The test–retest reliability was also very high: the intraclass correlation coefficient between the baseline PASE score and the score observed a few days after was 0.91 for the symptoms subscale, 0.92 for the function subscale, and 0.93 for the total score.
The convergent validity was measured comparing the PASE scores with those of the PEST, the VAS for pain and the other study questionnaires (Table II). Consistently with the results summarized in Table I, there is a moderate–high correlation with the PEST (0.63, 0.58, and 0.62 for the symptoms, function and total score, respectively) and the VAS for pain (0.52, 0.51, and 0.53 for the symptoms, function and total score, respectively). Interestingly, the correlation with the Skindex scores, although statistically significant, was low, and practically no correlation with the PASI scores was observed (0.04, 0.09, and 0.07 for the symptoms, function and total score, respectively).
Table II. Convergent validity: correlation between Psoriatic arthritis Screening and Evaluation (PASE) scores and other clinical and quality of life measures
|
PASE_SYM |
PASE_FUNC |
PASE_TOT |
|
|
PASE_SYM |
1 |
||
|
PASE_FUNC |
0.86** |
1 |
|
|
PASE_TOT |
0.96** |
0.97** |
1 |
|
PEST |
0.63** |
0.58** |
0.62** |
|
SKINDEX_29_SYM |
0.36** |
0.37** |
0.38** |
|
SKINDEX_29_EMO |
0.34** |
0.32** |
0.34** |
|
SKINDEX_29_FUN |
0.38** |
0.39** |
0.40** |
|
SKINDEX_17_SYM |
0.30** |
0.32** |
0.32** |
|
SKINDEX_17_PSY |
0.33** |
0.33** |
0.34** |
|
GHQ_CONTINUOUS |
0.38** |
0.40** |
0.41** |
|
GHQ_DICHOTOMOUS |
0.37** |
0.39** |
0.39** |
|
PASI |
0.04 |
0.09 |
0.07 |
|
Visual analogue scale pain |
0.52** |
0.51** |
0.53** |
SYM: symptoms; FUNC: function; FUN: social functioning; TOT: total; PASI: Psoriasis Area and Severity Score; PEST: Psoriasis Epidemiology Screening Tool; GHQ: General Health Questionnaire.
The PASE scores showed good responsiveness to clinical change over time.
Fig. 1A shows the mean differences (and 95% confidence intervals) between baseline and the 3-month follow-up scores, by evaluation of clinical change by the patients. A clear significant trend is observed with a 2.5 points improvement in the patients who reported they had “no or slight improvement”, a 3.2 improvement for those who reported “moderate improvement”, 7.3 for those who reported “substantial improvement”, and 14.2 for those who said they were “healed”. In Fig. 1B the mean changes over time for the 3 PASE scores are shown according to the presence of a diagnosis of PsA. For all 3 scales there is a highly statistically significant difference in the level of improvement according to whether the patients had or did not have PsA: 5.6 vs 1.6 for the Symptoms (p < 0.001); 4.5 vs 1.8 for the Function (p = 0.004); 10.2 vs 3.4 for the Total score (p < 0.001).
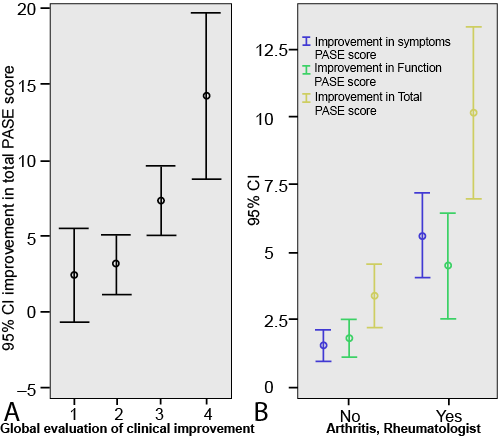
Fig. 1. Responsiveness of the Psoriatic arthritis Screening and Evaluation (PASE): mean differences (and 95% confidence intervals) between baseline and the 3-month follow-up. A: total PASE score by evaluation of clinical change by the patients. Clinical improvement scale: 1 = no/slight, 2 = moderate, 3 = good, 4 = very good/healed. B: Symptoms, Function, and Total PASE scores by presence of psoriasis arthritis.
A similar pattern was observed also both for the symptoms and the function subscale. All 3 scales had a p-value < 0.001 at the Wilcoxon test for paired samples.
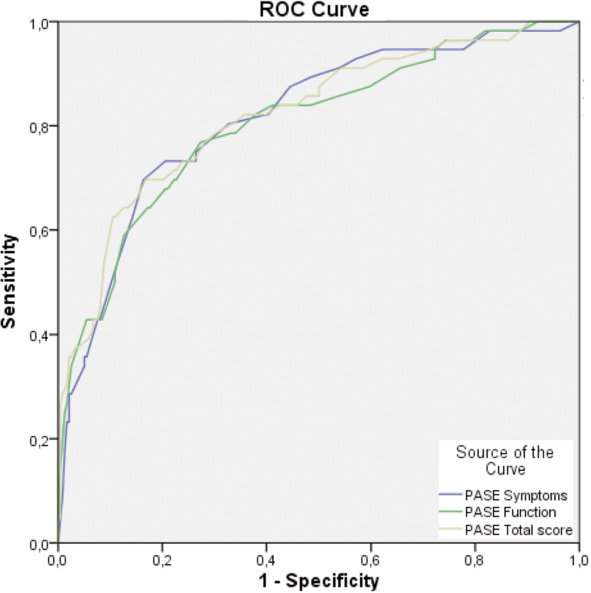
To determine the best cut-off value to identify patients with PsA we produced ROC curves for the two subscales and the total score of the PASE, using the rheumatologist’s diagnosis as outcome (Fig. 2). The area under the curve was always greater than 80%, and in particular: 81.6% for the symptoms, 80.4% for the function, and 82.1% for the total score. The optimal cut-off was found to be ≥ 48 on the total score, which was able to distinguish PsA from non-PsA patients with a 73.2% sensitivity and a 76.1% specificity.
Discussion
Our study shows that the PASE self-administered questionnaire may be a valid tool in helping dermatologists and other health care providers to screen for PsA. While this questionnaire is certainly not intended to establish by itself a diagnosis of PsA, we have found that using a cut-off of ≥ 48 on the total score it has good sensitivity and specificity in identifying patients with PsA who had been previously diagnosed by a rheumatologist. Such cut-off and such specificity and sensitivity values are surprisingly similar to those obtained by the authors of the original questionnaire (6). It is important to note that our study confirms a better performance of the PASE total score compared to the subscale scores (i.e., symptoms and function). These observations are particularly important because our Italian study population is certainly quite different, both in ethnic and cultural terms, from the population of the original studies.
The good field performance of the PASE questionnaire, in fact, is based on the solid results of the psychometric evaluation. The internal consistency was very satisfactory, with Cronbach’s alpha values of 0.90 or higher, and as high as 0.95 for the total score.
The observed scores in Table I are always supportive of a substantial construct validity, as they are consistently and significantly higher exactly where they should be, i.e., in patients with a greater clinician-rated clinical severity of disease, with a positive GHQ-12 score, and most importantly with a diagnosis of PsA (both according to a rheumatologist and to the CASPAR criteria).
Of particular interest is the comparison with the generic dermatological Skindex-29 questionnaire. In fact, the Skindex-29 scores do not show any significant difference between patients who have either a rheumatologist or a CASPAR diagnosis of PsA and those who do not. Also importantly, in the three categories of PASI score we used (from < 10 to ≥ 15) the Skindex-29 scores significantly increased with increasing PASI on the symptoms, emotions, and functioning subscales of this questionnaire. On the contrary, there is no difference whatsoever in PASE scores – indicating that the degree of skin involvement has a weak association with the severity of the PsA, and thus does not affect the scores of this PsA-specific questionnaire.
These observations are very important because they highlight the difference between valid questionnaires designed with different purposes (e.g., the Skindex-29 intended to measure the burden deriving by the skin involvement in different dermatological conditions and the PASE designed to evaluate PsA), and they warn us to use appropriately each questionnaire according to its intended target, and not to use one as the surrogate of the other.
While the PASE was designed essentially to stress its discriminative properties, i.e., to be used as a screening tool, in a subsequent paper Dominguez et al. (17) reported high levels of responsiveness for the PASE scores, and concluded that they may be used as a marker of therapeutic response.
We have confirmed also these results on the evaluative properties of the PASE by administering it over time and by linking the observed changes in scores to an overall evaluation of clinical improvement provided by the patients on a standardized scale. As shown in Fig. 1A, the PASE in our study showed an excellent sensitivity to clinical change. It may also be worthwhile noting that for the patients with PsA the improvement on the Function scale is less marked than on the Symptoms scale. Though such difference in our study does not reach statistical significance, it may indicate that dermatologists should be aware that a given improvement in their patients’ symptoms may not reflect directly in a functional improvement of the same magnitude.
As for most studies performed in a defined geo-cultural area, the main limitation of our study is that the results may not be generalizable to all countries, since populations with different cultural values (e.g, on pain, or on physical limitations in general) may respond differently to the questionnaire items. However, this problem is built-in in most patient-reported outcomes instruments, and our results – very similar to those of the original validation even if performed in a very different area and environment – should encourage other dermatologists to provide valid versions for their own languages.
In conclusion, our project shows that the use of the PASE questionnaires is possible in busy clinical routine practices and that its properties are stable and valid even when administered to patients with a very different ethnic and cultural background. Taken together, our results confirm that the PASE may help doctors – both in specialist dermatology settings and in general practices – to identify psoriasis patients with PsA and that it may be useful to monitor the course of the disease and to evaluate the effects of the prescribed treatments.
Acknowledgements
The authors wish to thank Patrizia Giannantoni, DStat, for performing part of the psychometric evaluation of the PASE.
Dr. Abeni has been supported, in part, by the “Progetto Ricerca Corrente” of the Italian Ministry of Health.
References

