


Departments of 1Dermatology,and 2Epidemiology and Biostatistics, CHU Hôtel-Dieu, 1 place A Ricordeau, FR-44093 Nantes cedex, France. *E-mail: sebastien.barbarot@chu-nantes.fr
Accepted Apr 27, 2017; Epub ahead of print Apr 27, 2017
Atopic dermatitis (AD) is the most common chronic inflammatory skin disease (1, 2). Systemic immunosuppressive treatments may be required for a minority of patients with recalcitrant severe disease. The strongest evidence for efficacy in patients with severe AD was obtained for cyclosporine A (CsA) (3), which is the only approved immunosuppressive treatment for this indication in Europe (4, 5). As novel biologic treatments are currently undergoing development for use in AD (6), it is of utmost importance to evaluate the effectiveness of CsA in a real-life setting in order to obtain a clear picture of the unmet needs in patients with severe AD.
Drug survival is the time patients remain on a specific drug (7). Performing drug survival studies with chronic diseases in a real-life setting is a way of assessing long-term drug effectiveness and safety. However, only one study has reported drug survival data for CsA in a long-term daily practice cohort of adult patients with AD (8). As the outcomes of drug survival studies may be influenced by specific behaviours of physicians and patients, it is important to replicate this study in other settings in order to establish the more general relevance of the findings.
The aim of the current study was to perform a detailed analysis of CsA modalities, effectiveness, and safety using drug survival analysis, as well as to examine which factors influence drug survival in AD.
A monocentric retrospective study was performed in a tertiary care regional health centre. All adult and paediatric patients with AD treated with at least one course of CsA with at least 2 visits from 1 January 2001 to 15 August 2015 were included. AD was defined according to the UK Working Party’s criteria (9). There was no minimal treatment duration. Patients could also receive local adjuvant treatments, but no oral adjuvant treatment. Data were collected from medical records from 1 May 2014 to 30 August 2015. As this was a retrospective epidemiological study, according to French legislation, approval from an ethics committee was not needed to use the data.
Patients’ follow-up was performed according to standard monitoring protocols (10).
The following data were recorded: date for the start and end of treatment, the Physician Global Assessment (PGA) (11), SCORing Atopic Dermatitis (SCORAD) score, treatment dosage, tolerance, adverse events (AE) and their grade according to Criteria for Adverse Events, as well as the reason to terminate treatment. The reasons to terminate treatment were assessed by the physician as being either due to remission, AE, or lack of efficacy of the treatment. A patient could have multiple reasons to terminate treatment. A complete remission was defined as a PGA 0 or 1. Follow-up duration was defined as the time from the start of treatment to the date of data-lock or loss to follow-up.
Quantitative data were displayed as means, medians and standard deviations (SD), and qualitative data as percentages. Drug survival was defined as the time (months) a patient remained on a specific drug. Kaplan–Meier survival curves were used to portray drug survival. Using a bivariate generalized linear model, we examined the influence of the following variables on the risk of discontinuation of CsA treatment: sex, age at start of treatment, AD severity at baseline, and initial dosage of CsA. Missing values were excluded from the analyses. Statistical analyses were performed with R software version 3.1.0.
A total of 88 patients (12 children) who received a first course of CsA during the study period (Table SI) were included. The mean ± SD age at the beginning of the treatment was 29.4 ± 12.3 years. The mean duration of follow-up was 26.7 months (range 0.3–154.7 months). At baseline, all patients had already received topical treatments, such as topical steroids (100%), topical calcineurin inhibitors (53.4%), or phototherapy (38.6%). All patients had received an individual education session prior to starting CsA. The mean ± SD SCORAD at the beginning of the treatment was 54.9 ± 15.2).
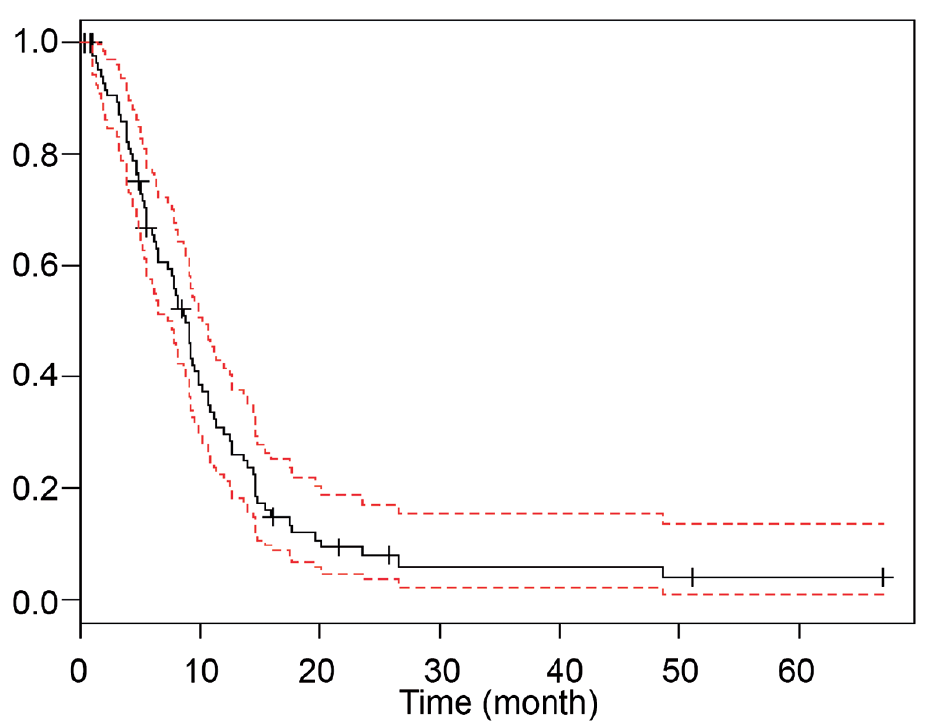
Overall, the median duration of CsA treatment was 8.23 months (range 1–49.5 months). The mean starting dose was 3.6 mg/kg/day. Fifty patients (56.8%) had the following AE: gastrointestinal symptoms (14.8%), neurological symptoms (14.8%), arterial hypertension (11.3%), or an increase in serum creatinine level (11.3%) (Table SI). CsA survival rates were 67.0% at 6 months and 34.1% at 12 months (Fig. 1). Twenty-two patients (25%) were in complete remission at the first follow-up visit (a mean of 2.4 months), and 16 (18.2%) at the time of the second follow-up visit (a mean of 5.6 months).
Fig. 1. Cyclosporine A (CsA) overall survival rates in time (in months; black curve) Red curved represents a 95% confidence interval. CsA survival rates were 90.9% at 3 months, 67.0% at 6 months and 34.1% at 12 months.
At the time of data lock, 77 patients (87.5%) had stopped treatment: 40 (45.5%) due to remission, 20 (22.7%) due to AE, and 20 (22.7%) due to lack of efficacy of the treatment. Two patients were still on treatment.
There were no associations between the tested variables (i.e. sex, age at the beginning of the treatment, AD severity at baseline) and reasons to stop treatment with CsA (remission, lack of efficacy or AE) (Table SII). An association was shown between the initial dosage of CsA and discontinuation of the treatment due to AE. Indeed, a CsA starting dose of > 3.5 mg/kg/day was associated with an increased risk of discontinuation related to AE (odds ratio (OR) 5.86, confidence interval (CI) 1.74–27.04; p = 0.009).
This retrospective study included 88 patients with AD who received a first course of CsA for insufficient control of their disease. Only 25% of the patients were in complete remission at the first follow-up visit in this study.
Drug survival analyses are important to describe daily practice treatments in dermatology (8, 12), although they are still rarely used. To our knowledge, this is the second published study reporting on modalities of CsA treatment for severe AD in a cohort of patients using drug survival analysis. Recently, Van der Schaft et al. (8) published a drug survival study for CsA in a cohort of 356 adults with AD. In this study, 22% of the patients terminated their treatment due to AE, and 16% due to ineffectiveness of the treatment. These results are in keeping with our findings. We confirm that the rates of discontinuation due to AE in real life are higher than in clinical trials (8, 13–15). Indeed, short follow-up periods and selection bias in clinical trials preclude proper assessment of the long-term safety of treatments.
We found that 45.5% of patients in the current study stopped CsA treatment due to remission. This proportion is higher than was reported in the study by Van der Schaft (26.4%). It may reflect a higher effectiveness of CsA in the cohort in the current study, or particular behaviours of the physicians.
Contrary to Van der Schaft’s results (8), a CsA starting dose >3.5 mg/kg/day was not associated with a higher effectiveness in the current study. Rather, it was associated with an increased risk of discontinuation that was related to AE. Physicians should be aware of the potential AE of this drug in non-selected patients with comorbidities.
The results of this study should be interpreted with caution due to the retrospective design; however, we conclude that a daily dose of cyclosporine > 3.5 mg/kg may be harmful, with no additional benefit in a real-life setting.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize