


1Centre for Pharmacoepidemiology, Karolinska Institutet, 2Division of Internal Medicine, Danderyd Hospital, Stockholm, 3Department of Dermatology and Venereology, Bispebjerg University Hospital, Copenhagen, and 4Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark
*These authors contributed equally.
Studies on pregnancy and birth outcomes in women with psoriasis are scarce and the findings inconsistent. The effect of maternal psoriasis and its severity on the risk of adverse pregnancy and birth outcomes was examined. A cross-national population-based cohort study was performed using prospectively collected data from Denmark and Sweden. Singleton births in women with psoriasis were identified in the national health registers between April 2007 and December 2012 and classified according to disease severity. Lifestyle factors, co-morbidity, pregnancy and birth outcomes were evaluated. A total of 8,097 births were identified in 6,103 women with psoriasis and 964 births in 753 women with psoriatic arthritis. Increased risk of gestational diabetes, gestational hypertension, pre-eclampsia, elective and emergency caesarean delivery was found in women with psoriasis. The risks were higher for women with severe psoriasis, who also had an increased risk of preterm birth and low birth weight. Pre-conception counselling to improve maternal, pregnancy and birth outcome is encouraged.
Key words: psoriasis; adverse pregnancy and birth events; observational study.
Accepted Mar 15, 2018; Epub ahead of print Mar 15, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Ann Haerskjold, Department of Dermatology and Venereology, Bispebjerg University Hospital, Bispebjergbakke 23, DK-2400 Copenhagen, Denmark. E-mail: annhaerskjold@gmail.com
Psoriasis is a common chronic inflammatory disorder with significant physical and psychological sequelae. This study evaluated pregnancy and birth outcomes in Danish and Swedish women with psoriasis. Increased risk of gestational diabetes, gestational hypertension, pre-eclampsia, elective and emergency caesarean delivery was found in women with psoriasis. The risks were higher for women with severe psoriasis, who also had an increased risk of preterm birth and low birth weight. Pre-conception counselling to improve maternal, pregnancy and birth outcome is encouraged.
Psoriasis is a complex chronic inflammatory disease. Its pathophysiology is not fully understood, but involves genetic, immunological, environmental, and lifestyle-related factors. The prevalence of psoriasis in women of reproductive age is approximately 1% (1).
A substantial proportion of patients with psoriasis develop obesity, hypertension, diabetes mellitus, depression and other chronic inflammatory diseases, such as inflammatory bowel disease (IBD) and rheumatoid arthritis (RA) (2, 3), all of which have been associated with adverse pregnancy and birth outcomes. Joint symptoms are common among patients with psoriasis and 6–30% develop psoriatic arthritis (PsA) (3). Furthermore, patients with psoriasis are more prone to a generally unhealthy lifestyle, including smoking, which is also associated with adverse pregnancy and birth outcomes (4, 5).
Large population-based studies on pregnancy and birth outcomes in women with psoriasis are scarce, and the results of previous studies are inconsistent (6–10). The aim of this study was to assess the effect of maternal psoriasis and its severity on adverse pregnancy and birth outcomes using a population-based register data in Sweden and Denmark.
This observational population-based cohort study used data from the national birth registers (11), the national patient registers, and the national prescribed drug registers (12–15) in Denmark and Sweden. The national birth registers include data on maternal characteristics (age at delivery, parity, smoking habits, body mass index (BMI)) and on pregnancy, delivery and the neonatal period. The patient registers contain information on all hospitalizations and outpatient visits to specialist care, including primary and secondary diagnoses. Diagnoses are recorded according to the International Classification of Diseases, version 10 (ICD-10) and data are available from 1998 onwards in Sweden and Denmark. The prescribed drug registers include data on the formulations and date of all dispensed prescriptions. Drugs are categorized according to the WHO Anatomical Therapeutic Chemical classification (ATC codes). In Denmark, data on prescribed drugs have been available since 1999 and in Sweden since July 2005. Individual record linkage between the registers in each country is possible through the unique personal identification number assigned to all residents at birth or immigration.
The study was approved by the Regional Ethical Review Board at Karolinska Institutet, Stockholm, Sweden (record number 2006/889:31).
All women who gave birth to a singleton infant in Denmark and Sweden from 1 April 2007 to 31 December 2012 were identified. Some women gave birth more than once during the study period and each birth was considered individually. Women with psoriasis were identified either by an ICD-10 code (L40 (excluding PsA L405, M070–M073), or by at least one dispensed prescription of calcipotriol (D05AX02) and/or calcipotriol in combination with betamethasone (D05AX52), systemic anti-psoriatic drugs (D05B) or mometasone in combination with salicylic acid (D07XC03) before or during pregnancy. Women with a diagnosis of PsA (L405, M070–M073) were defined in a separate cohort. All other women in the study were categorized as women without psoriasis.
Women with psoriasis were further categorized according to disease severity. Severe psoriasis was defined by: systemic drug administration with at least one dispensed prescription of any of the following drugs: methotrexate (L04AX03), and/or ciclosporin (L04AD01), systemic anti-psoriatic treatment (D05B) and/or biologic agents anti-tumour necrosis factor (anti-tumour necrosis factor; anti-TNF), ustekinumab, efalizumab, abatacept, leflunomide (L04AB, L04AC05, L04AA21, L04AA24, L04AA13) before or during pregnancy.
Non-severe psoriasis was defined by the use of anti-psoriatic topical drugs only, or a diagnosis of psoriasis without recorded treatment.
Adverse pregnancy and birth outcomes were identified from data obtained from the medical birth registers and the patient registers in Denmark and Sweden. Pregnancy outcomes included: gestational diabetes (O244), gestational hypertension (O13), antenatal haemorrhage (O45–O46), venous thromboembolism (I26, I80–82, O22) during pregnancy, and pre-eclampsia (O11, O14–O15). Only women without prescriptions of anti-diabetic and anti-hypertensive medications up to one year prior to pregnancy were eligible to develop gestational diabetes or hypertension, respectively. Thus, women with antidiabetic and antihypertensive medication prescriptions less than 1 year prior to pregnancy were not eligible to develop the outcomes gestational hypertension and gestational diabetes, respectively. Adverse birth outcomes included: delivery by elective or emergency caesarean section, preterm birth (< 37 weeks of gestation), moderate preterm birth and very preterm birth (32–36 and < 32 weeks of gestation, respectively), low Apgar score (< 7), being small for gestational age (SGA), low birth weight (≤ 2,500 g), stillbirth and major congenital malformations (Q00–Q99). Stillbirth in the Danish medical birth register includes infants born after 22 weeks of gestation. In Sweden, the same cut-off has been used since July 2008, prior to which gestational week 28 was used. All conditions were dichotomized (yes/no) in the analyses.
As co-variates, we included conditions recorded in the national health registers. These covariates were: maternal age (13–19, 20–24, 25–29, 30–34, ≥ 35 years), parity (primiparous/multiparous), country (Denmark/Sweden), smoking (yes/no), body mass index (BMI) (≤ 18.4, 18.5–24.9, 25–29.9, ≥ 30), hypertension (yes/no), diabetes (yes/no) and depression (yes/no). These were identified from the patients’ register and the prescribed drug registers with ICD-10 codes and ATC; hypertension (ICD-10: I10–I13, ATC: C02–C03, C07, C09), diabetes mellitus (ICD-10: E10–E11, ATC: A10) and depression (ICD-10: F32, F33, ATC: N06A).
Analyses were performed using SAS software, version 9.3 (SAS Institute Inc., Cary, NC, USA). Logistic regression was used to compare the association of adverse pregnancy and birth outcomes between women with psoriasis and women without psoriasis. The associations are presented as crude odds ratios (ORs) and adjusted odds ratios (aORs) with 95% confidence intervals (CIs). Using logistic regression, the ORs were adjusted in 2 multivariable models. The first model (Model 1) was adjusted for country, maternal age and parity. The second model (Model 2) was also adjusted for smoking, BMI, depression, diabetes and hypertension. To assess the impact of severity of psoriasis on the adverse pregnancy and birth outcomes, separate analyses were performed comparing women with severe and non-severe psoriasis with women without psoriasis. Furthermore, absolute risks were estimated and presented as number of attributable cases.
In sensitivity analyses, psoriasis was re-defined, requiring at least one recorded diagnosis of psoriasis by ICD-10 code and separately requiring a diagnosis within the 5 years prior to the start of the pregnancy to determine the exposure. In another analysis, the women on systemic anti-psoriatic treatment during pregnancy were excluded (data on request). To address misclassification of PsA/RA sensitivity analyses were also performed of PsA, excluding women who had a diagnosis of RA after their latest PsA diagnosis, and more frequent RA diagnoses than PsA diagnoses. Sensitivity analyses with BMI and maternal age as continuous variables were performed (Tables SI–SIII).
A total of 741,973 women with 952,907 pregnancies were included during the study period, of whom 608,372 (68%) were from Sweden and 344,535 (32%) from Denmark. In 8,097 (0.9%) of the pregnancies, the criteria for psoriasis was met, and of these 312 (4%) of the pregnancies were categorized as severe psoriasis cases, while 964 (11%) pregnancies fulfilled the criteria of PsA.
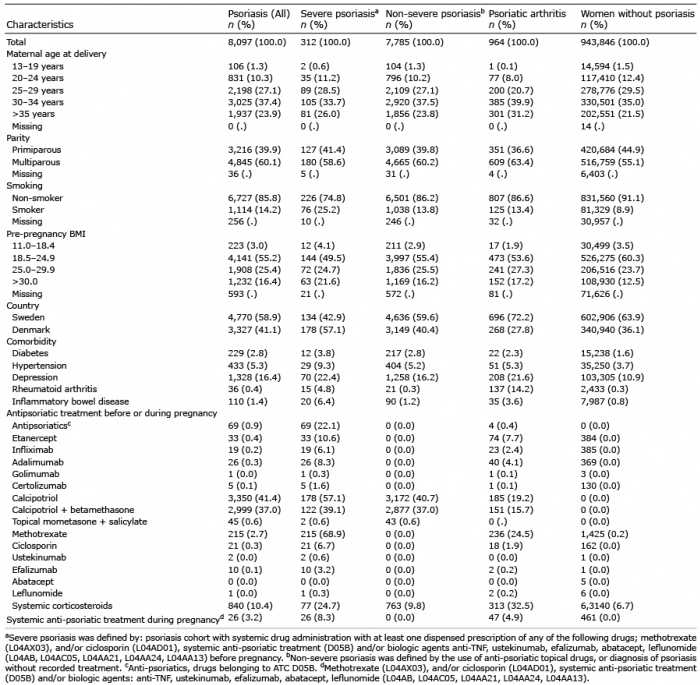
Baseline characteristics of the pregnancies in women with and without psoriasis, and prescribed drugs before and during pregnancy are shown in Table I. Women with psoriasis and PsA were older and more frequently had a high pre-pregnancy BMI (Table I and Table SIV). They were more often smokers and more often diagnosed with diabetes, hypertension, and depression, compared with women without psoriasis. The differences were more pronounced in women with severe psoriasis and women with PsA, than among those with non-severe psoriasis. Newborns of women with psoriasis were more likely to have a higher Apgar compared with healthy women (Table II). Co-morbidity as RA and IBD was more common in those categorized as having PsA.
Table I. Maternal characteristics of singleton births with psoriasis (all and by severity), with psoriatic arthritis and without psoriasis or psoriatic arthritis, in Denmark and Sweden between 1 April 2007 and 31 December 2012
Table II. Risk of adverse pregnancy and birth events in singleton pregnancies with and without psoriasis. Pregnancies without psoriasis serves as reference
When adjusting for maternal age, parity and country (Model 1), we found an increased risk of gestational diabetes (aOR 1.36, 95% CI 1.18–1.57), gestational hypertension (aOR 1.26, 95% CI 1.10–1.44) and pre-eclampsia (aOR 1.28, 95% CI 1.14–1.44) in pregnancies in women with psoriasis. In addition, women with psoriasis had increased risks of elective caesarean section (aOR 1.17, 95% CI 1.08–1.26) and emergency caesarean section (aOR 1.16, 95% CI 1.08–1.26) (Table II). The absolute risks of gestational diabetes and gestational hypertension were 7 and 6 per 1,000 women, respectively. The corresponding numbers for pre-eclampsia, elective and emergency section were 9, 13 and 13, respectively.
In Model 2, in which we adjusted for all co-variates, we found increased risks of gestational diabetes (aOR 1.20, 95% CI 1.02–1.40), gestational hypertension (aOR 1.17, 95% CI 1.02–1.35) and pre-eclampsia (aOR 1.15, 95% CI 1.01–1.30) in women with psoriasis. Furthermore, there was an increased risk of delivery by elective caesarean section (aOR 1.11, 95% CI 1.02–1.20) or emergency caesarean section (aOR 1.09, 95% CI 1.01–1.18). The absolute risks of gestational diabetes and gestational hypertension were 4 in 1,000 women. The corresponding numbers for pre-eclampsia, elective and emergency section were 5, 9 and 8, respectively.
Children of women with psoriasis had higher Apgar score compared with women without psoriasis. However, the association was not significant. For both models, no increased risks of antepartum haemorrhage, venous thromboembolism, preterm birth, SGA, stillbirth or major congenital malformations were found in women with psoriasis. Changing the definition of psoriasis to require a recorded diagnosis and excluding the women who had systemic treatment during pregnancy did not change the results (data available on request).
Risks of adverse pregnancy and birth outcomes in women with severe psoriasis are presented in Table III. In model 2, we found further increased estimates for gestational hypertension (aOR 2.22, 95% CI 1.22–3.68), pre-eclampsia (aOR 1.69, 95% CI 1.02–2.82), moderate preterm birth (aOR 1.64, 95% CI 1.03–2.61.) and low birth weight (aOR 1.81, 95% CI 1.14–2.89). The absolute risks found for gestational diabetes, gestational hypertension and pre-eclampsia were 12, 25 and 21 per 1,000, respectively. The corresponding numbers for preterm birth, elective and emergency section and low birth weight were 25, 27, 34 and 26, respectively. Women with PsA had increased risk of gestational hypertension (aOR 1.60, 95% CI 1.13–2.29), pre-eclampsia (aOR 1.49, 95% CI 1.08–2.05) and delivery by elective caesarean section (aOR 1.49, 95% CI 1.18–1.81) (Table IV).
Table III. Risk of adverse events in singleton pregnancies by severity of psoriasis (non-severe and severe psoriasis). Pregnancies without psoriasis serves as reference
Table IV. Risk of adverse events in singleton pregnancies, psoriatic arthritisa (n = 964). Pregnancies without psoriasis serves as reference
In this population-based study, including all singleton births in Sweden and Denmark from 1 April 2007 to 31 December 2012, we found increased risks of gestational diabetes, gestational hypertension, pre-eclampsia, and elective and emergency caesarean section among women with psoriasis compared with women without psoriasis. The associations were stronger among women with severe psoriasis, who also had increased risks of preterm birth and low birth weight. Women with PsA had increased risk of gestational hypertension, pre-eclampsia and delivery by elective caesarean section.
The associations between psoriasis and gestational diabetes and gestational hypertension have not been reported previously. Both gestational diabetes and gestational hypertension have been linked to the development of diabetes and cardiovascular disease later in life, suggesting the benefits of preventive measures in this group (16, 17). In our study, women with psoriasis had an increased risk of pre-eclampsia, regardless of severity, though this tendency was stronger in women with severe psoriasis and PsA. The finding of increased risk of pre-eclampsia in women with severe psoriasis is in line with a previous population-based study by Yang et al. (18), who compared 1,483 pregnant women with psoriasis with 11,704 pregnant women without psoriasis. The authors found a positive correlation between severe psoriasis and pre-eclampsia. However, mild psoriasis was not associated with pre-eclampsia. These different findings may be explained by a relatively limited number of psoriasis patients in the previous study, and the different definitions of psoriasis severity used.
Women with psoriasis had an increased risk of birth by elective or emergency caesarean section. In 2 previous studies, no association was found between psoriasis and caesarean delivery, while another study found psoriasis to be an independent risk factor for caesarean delivery (6, 10, 18). The increased risk of caesarean section may be attributed in part to a high BMI and depression among those with psoriasis, since both BMI and depression are independently linked to delivery by caesarean section (19, 20). The association, however, did not disappear in the fully adjusted analysis, which may imply that the effect of psoriasis on caesarean section is not exclusively related to these conditions.
Preterm birth is associated with increased morbidity and mortality both early and later in life (21, 22). Our finding of increased risk of preterm birth among those with severe psoriasis has not been reported previously. The higher risk of preterm birth was observed mainly for moderate preterm birth, which is reassuring, since the risks for the infant decline with higher gestational age at birth. We found no increased risk of antepartum haemorrhage, venous thromboembolism, Apgar <7, and congenital malformation. These findings are in line with earlier findings (23).
The finding of increased risk of gestational hypertension, pre-eclampsia and delivery by elective caesarean section in women with PsA has not been reported previously. However, co-morbidity as RA and IBD was more frequent in women with PsA. Both conditions have been linked to adverse pregnancy and birth outcomes (24, 25). The increased risk of adverse pregnancy outcomes in women with PsA may also be attributed partly to a high pre-pregnancy BMI, hypertension and depression among those with PsA. The association, however, persisted in the fully adjusted analyses and in sensitivity analyses, which may imply that the effect is not exclusively related to these conditions.
Obesity, diabetes, hypertension and depression were more common among women with psoriasis in this study, particularly among those with severe psoriasis and PsA. These findings are in accordance with a previous study (26) and all these conditions have previously been associated with increased risks of adverse pregnancy and birth outcomes. The co-existence of psoriasis and obesity is, at least in part, attributed to the regulation of adipokines secreted by the visceral fat. High levels of TNF and interleukin 6 (IL-6), present in both psoriasis and obesity, have been associated with insulin resistance and diabetes. Obesity is already seen at a young age, and the fat is often more centrally, rather than generally distributed in patients with psoriasis. The presence of central adiposity in early life suggests that the obesity may, in part, be genetically determined (27–29). Also, obesity is a risk factor for severe psoriasis and it may trigger psoriasis development in genetically susceptible individuals (30). In addition, weight reduction may improve psoriasis symptoms (31). Depression is suspected to be an independent risk factor for the development of psoriasis, and the inflammatory pathways of psoriasis and depression are similar (32, 33). Smoking, which may trigger the development of psoriasis (34, 35), was observed more frequently among women with psoriasis in this study, illustrating the unhealthy lifestyle previously linked to psoriasis. BMI, hypertension, diabetes and depression are confounding factors, but may also be considered as causal intermediates that lie on the pathway through which psoriasis exerts its effects. Thus, we found it appropriate to present both models. The attenuation of the risks, when adjusting for these conditions, indicate that lifestyle changes may potentially reduce risks of adverse pregnancy and birth outcomes.
The management of psoriasis and PsA in pregnant women is challenging, since the physician and patient must balance teratogenic risks associated with certain drug therapies with potential adverse pregnancy outcomes from uncontrolled skin and joint inflammation. Use of systemic anti-psoriatic drugs during pregnancy may be unavoidable in a limited proportion of women with psoriasis. Some anti-psoriatic drugs, e.g. methotrexate, have been found to negatively affect pregnancy and birth outcomes. It was not possible to study the effect of drug exposure during pregnancy as too few women were exposed: only 73 women had a prescription of any systemic anti-psoriatic drug during pregnancy. When excluding these women from the analysis, estimates remained unchanged.
A major strength of this study is its large size and population-based design, comprising all singleton births during the study period in Sweden and Denmark, which makes it feasible to study multiple and rare outcomes, and limits selection bias. Furthermore, adjustments for potential confounding factors were made in regression analyses using available data. However, the risk of bias may still exist, as some factors (e.g. genetic factors) are not accounted for in epidemiological studies.
Data were not collected primarily for research purposes and misclassification may exist. However, potential misclassification is most likely non-differential, leading to bias towards the null.
A high proportion of women with PsA also had a diagnosis of RA. We therefore ran sensitivity analyses to assess the impact of potential misclassification of RA vs. PsA. This had minor effects on the results for the PsA cohort, showing slightly lower point estimates, but may have removed some bias from misclassification.
Changing the definition of psoriasis in sensitivity analyses did not change the results. Systemic drug treatment and a diagnosis of psoriatic arthritis were used as a proxy for severe disease, which may incorrectly classify some women with severe psoriasis as non-severe, again leading to a dilution of risks. However, the use of systemic treatment and/or being diagnosed with psoriatic arthritis generally reflects a severe disease course. It was not possible to compare this with clinical data on psoriasis severity, e.g. Psoriasis Area Severity Index (PASI).
Pregnant women with psoriasis and PsA more often exhibit an unhealthy lifestyle and are at increased risk of adverse pregnancy and birth outcomes. Modifiable lifestyle factors should be addressed in women with psoriasis who are of childbearing age.


 Click to show fullsize
Click to show fullsize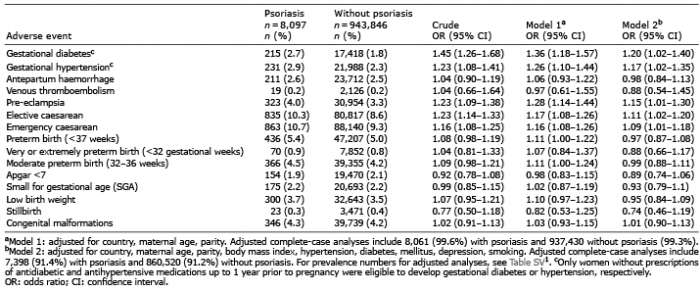 Click to show fullsize
Click to show fullsize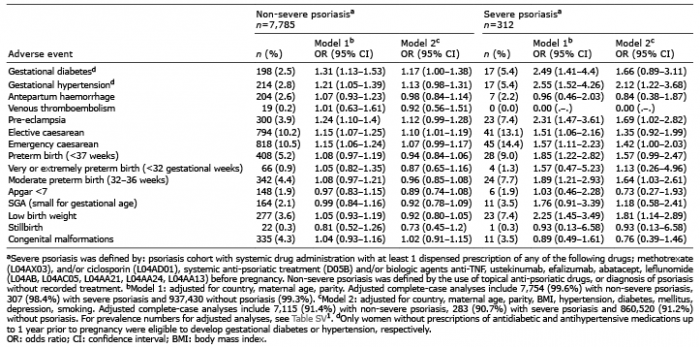 Click to show fullsize
Click to show fullsize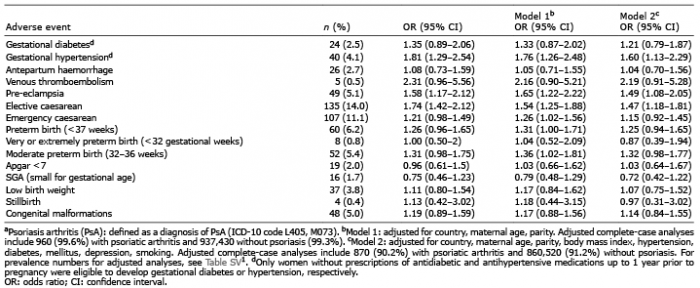 Click to show fullsize
Click to show fullsize