


1Department of Dermatology, 2Laboratory of Immunology and Immunotherapy, INSERM U1227, 3Department of Internal Medicine, Pneumology and Vascular Medicine, and 4Department of Rheumatology, INSERM U1227, CHRU Brest, Brest, France
#These authors have contributed equally as senior authors.
Pruritus is a frequent symptom in systemic sclerosis (SSc), with a prevalence of 40–65%, but its patho-physiology is poorly understood. This study investigated the immunological component of pruritus. Fifty-six patients with SSc responded to a standardized questionnaire regarding both SSc disease and pruritus characteristics. Among patients with SSc, those with pruritus did not display a particular immunological profile (inflammatory, humoral, and/or cellular factors), but pruritus was, in most cases, concomitant with the development of SSc. Thus, pruritus characteristics were evaluated further, according to the detection of anti-centromere autoantibodies (ACA), into ACA+ (n = 17) and ACA– (n = 19). The ACA+ subgroup was characterized by a longer evolution of SSc and pruritus, pruritus present outside the sclerotic area, and a shorter daily duration of pruritus. In conclusion, the concomitant appearance of the 2 processes and the differences observed between ACA+ and ACA– subgroups support the presence of an immunological component in pruritus.
Key words: systemic sclerosis; pruritus; itch; autoantibodies; inflammation; autoimmunity; quality of life.
Accepted May 29, 2018; Epub ahead of print Jun 1, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Yves Renaudineau, Laboratory of Immunology and Immunotherapy, Brest University Medical School Hospital, BP 824, FR-29609, Brest, France. E-mail: yves.renaudineau@univ-brest.fr
Key points related to the study:
- Systemic sclerosis and pruritus appear in most of the cases concomitantly.
- This study unmasks different characteristics of pruritus according to the autoimmune subtype of systemic sclerosis.
- Pruritus characteristics are less severe when anti-centromere antibodies are detected.
Systemic sclerosis (SSc) is a rare and complex autoimmune connective tissue disease characterized by vascular changes and fibrosis of the skin and viscera, resulting in organ failure and irreversible injury (1). The disease process starts with vascular injury and endothelial activation, leading, in turn, to an uncontrolled inflammatory reaction, which triggers fibroblast activation (2, 3). In this complex disease, environmental factors (e.g. exposure to silica and solvent) seem to be the main factors in genetically primed individuals (4). In addition, recent results from genome-wide association studies (GWAS) have further shown different SSc subtypes confined to specific autoantibody profiles, including anti-centromere antibodies (ACA) or anti-topoisomerase/scl70 antibodies (5). The prevalence of SSc, ranging from 150 to 443 cases per million, vary substantially in different regions of the world, with higher reports in North America and Australia compared with Japan and France (6). A sex bias toward women is observed in SSc (female to male sex ratio approximately 4:1).
The most common organ complications associated with SSc are gastrointestinal (90%) followed by musculoskeletal problems (65%), interstitial lung disease (40%), pulmonary arterial hypertension (15%) and renal crisis (5–10%). Regarding skin involvement, SSc is characterized by skin fibrosis (> 90%), Raynaud’s phenomenon (90%), telangiectasia (75%), ulcers (40%) and calcinosis (25%) (1). Chronic pruritus represents a common, but infrequently reported, skin symptom in SSc, with a prevalence of 43–62% (7–9), compared with 7–14% for chronic pruritus in the general population (10–13). In primary care consultations, pruritus represents the main complaint in 0.6–1.0% of cases (13–15).
Pruritus, or itch, is defined as “an unpleasant sensation, which provokes the desire to scratch” (16). This unpleasant sensory experience is difficult to explore due to its multidimensional aspects, including sensory, cognitive, affective and motivational components (17). From the neurological point of view, 2 types of unmyelinated fibres leading to pruritus are described (18). First, histamine-sensitive fibres have an important role in the transmission of most types of acute pruritus, including urticaria. Secondly, non-histamine-sensitive peripheral C-nerve fibres are involved in the transmission of most types of chronic pruritus. Of particular note, these pruriceptors are distinct from the C-nerve fibres that transmit pain (nociceptors). Emerging arguments further support the possibility of cross-talk between the sensory nervous system and the immune signalling pathways to influence mammalian behaviour through the emergence of neurophysiological reflexes, especially on the skin with the scratching reflex, to expel invading pathogens and noxious environmental stimuli (18).
Thus, we have further hypothesized that activation of the immune system in autoimmune disease conditions with significant skin involvement, such as SSc, may contribute, either directly or indirectly, to pruritus. This is the question addressed by the present study.
Patients 18 years and older followed for SSc between 2000 and 2015 in the Departments of Dermatology, Rheumatology, Internal Medicine and Pneumology at Brest University Medical School, Brest, France, and referenced in the hospital register were invited to respond retrospectively to a standardized questionnaire dealing with the main characteristics of SSc and pruritus at disease initiation and at the time of the questionnaire. In parallel, we retrospectively collected biological data and information regarding digestive, renal, pulmonary, musculoskeletal and haematological complications through the analysis of hospitalization and consultation reports. Patients were classified as having diffuse or limited cutaneous SSc, based on the classification of LeRoy et al. (19). The CREST Syndrome (Calcinosis, Raynaud’s phenomenon, Esophageal dysmotility, Sclerodactyly, Telangiectasia Syndrome) is included in the limited cutaneous SSc. All the individuals included in this study have been described previously (7). The questionnaire, protocol presentation and a consent form were sent to patients following approval of the study by the local ethics committee.
Patients were first asked whether they had pruritus, and if the response was “yes”, they were invited to complete a 2-part questionnaire. The first part is specific for SSc and related to the duration of the disease, and topography of skin involvement. The second part of the questionnaire about pruritus, known as the “Brest questionnaire”, previously used in studies of other dermatoses (7, 20, 21), deals with intensity, chronology, location, characteristics of pruritus, and other associated sensations. The severity of pruritus was also evaluated using the score elaborated by Elman et al. in 2010 (22), the 5-D itch scale that uses 5 items (duration, intensity, evolution, impact on daily activities and location). The impact of the pruritus on quality of life (QoL) was studied by questions exploring the impact of pruritus on daily activities and by using the validated 22-question-based pruritus-specific questionnaire, ItchyQoL (23).
Biological data were recovered from 56 patients. These data dealt with inflammation (erythrocyte sedimentation rates (ESR), fibrinogen, C-reactive protein (CRP), haemoglobin, platelets, leukocytes), humoral immunity (total immunoglobulins IgG, IgA, IgM), complement factors (CH50, C3c, C4), and cellular immunity (lymphocyte subsets). The autoantibody (Ab) profile was comprised of the anti-nuclear Ab (ANA) and anti-centromere Ab (ACA) determination on HEp-2 cells, anti-Scl70 Ab, anti-SSA/Ro 52+60kDa Ab, anti-SSB/La Ab, rheumatoid factor (RF), and anti-cardiolipin Ab (aCL, IgM and IgG), as reported previously (24). Values above the laboratory standard were considered positive and, when several assessments were available, we selected those that were close to the date of the questionnaire (range 1–24 months).
Continuous data are described as mean ± standard deviation (SD). Differences among groups were analysed with the Kruskal–Wallis test, or the Fisher’s exact test for categorical data. Nominal values were compared with controls using the non-parametric Mann–Whitney rank sum test. p-values under 0.05 were considered significant. Statistical analysis was performed using GraphPad Prism 7.0 (La Jolla, CA, USA).
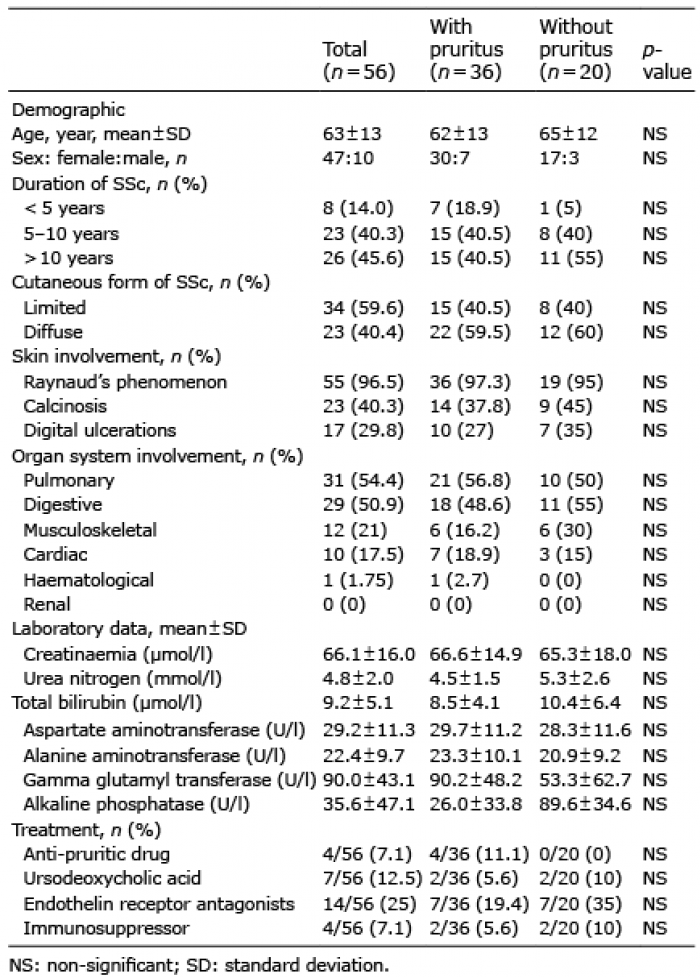
A list of 137 patients with SSc was established by the Medical Registry Department at Brest University Medical School from January 2000 to November 2015 (Fig. S1). Deceased patients (n = 55) were excluded from the study. The questionnaire was then sent to 82 patients, 56/82 (68.3%) were selected, while the others 26/82 (31.7%) were not included due to missing responses to the questionnaire (n = 13), refusal to participate (n = 8), or to the absence of biological data (n = 5). Pruritus was reported in 36/56 (64.3%) of the cases of SSc. Next, and when comparing patients with or without pruritus (Table I), no differences were highlighted between both groups with regards to age, sex, disease duration, SSc form, and organ involvement including skin.
Table I. Comparison of features in patients with systemic sclerosis (SSc) with or without pruritus
The question as to whether pruritus is associated with immunological parameters (Table II) was then addressed. Thus, several immunological parameters were evaluated, including parameters related to inflammation (ESR, fibrinogen, CRP, haemoglobin, platelets, leukocytes), complement activation (CH50, C3c, C4), immunoglobulin levels (IgG, IgA, and IgM), auto-antibody status (e.g. ANA, ACA, Scl70, SSA/Ro, SSB/La, RF, aCL) and lymphocyte subsets. None of these parameters were associated with the development of pruritus in patients with SSc. It was concluded from this analysis that pruritus could not be associated with a particular immunological profile; however, such negative observations do not exclude the possibility that part of the pathophysiological or semiological characteristics of pruritus may be linked with an immunological component.
Table II. Immunological characteristics in patients with systemic sclerosis (SSc) with or without pruritus
Next, and in order to test such an hypothesis (Table III), we further considered 2 subgroups of patients with pruritus based on ACA detection (group 1: ACA+ n = 17; group 2: ACA– including 4/19 with anti-Scl70 Ab) as important demographic, clinical and genetic differences were reported between these 2 subgroups (1). Indeed, patients in the pruritus ACA+ SSc subgroup were older (67.5 ± 12 years in SSc ACA+ vs. 57 ± 13 years in SSc ACA–, p = 0.015), presented a longer disease duration (p = 0.009, Fig 1A), and, as expected, sclerosis was limited in all ACA+ SSc patients, while only 26% had a limited form in the ACA– SSc subgroup. The same analysis conducted in patients without pruritus revealed an association only between limited SSc and ACA positivity.
Table III. Demographic and clinical characteristics of patients with systemic sclerosis (SSc) according to the autoimmune status
Fig. 1. Disease onset and pruritus are usually concomitant in patients with systemic sclerosis (SSc). Comparison of time elapsed since the onset of (A) SSc and (B) pruritus according to the autoimmune status of the patients. (C) Pruritus appearance according to onset of SSc. Results are expressed as a percentage of patients and indicated as significant when p < 0.05. ACA: anti-centromere antibodies.
With regards to parameters associated with pruritus between both groups of patients with SSc, it was first established that ACA+ SSc patients presented a longer duration of pruritus (p = 0.009, Fig 1B and Table IV). As extended disease duration is also important in the ACA+ SSc subgroup, this supports a concomitant appearance of SSc and pruritus in both subgroups. In the ACA+ SSc subgroup, pruritus pre-existed the SSc in 17.6% (3/17) of cases, 47.1% (8/17) of cases had concomitant appearance of pruritus and cutaneous scleroderma, and 35.3% (6/17) of cases reported a subsequent appearance (Fig 1C). In the ACA– SSc subgroup, both events were predominantly concomitant in 84.2% (16/19) of cases, while subsequent in the other cases (15.8%). Secondly, we further explored the mode of presentation at onset (progressive or abrupt), and the fluctuation of pruritus (intermittent, permanent, circadian rhythms) showing similarities between ACA+ and ACA– SSc subgroups. Thirdly, concerning the parameters of pruritus per day (Fig. 2A/B), the ACA+ SSc subgroup was characterized by a lower intensity with regards to 3 of the 6 criteria studied (qualitative scale discrete to moderate vs. severe to unbearable, p = 0.02); quantitative scale, p = 0.04 and p = 0.05 for criteria now and average, respectively; but not the 5-D itch scale, NS), and a shorter duration of pruritus per day (p = 0.05, Fig. 2C). Fourthly, pruritus occurred predominantly in the non-sclerotic area (82.4%) when considering the ACA+ SSc subgroup, while it was the sclerotic area (63.2%) that predominates in the ACA– SSc subgroup (p = 0.006) (Fig. 2D).
Table IV. Comparison of pruritus characteristics in patients with systemic sclerosis (SSc) according to their autoimmune status
Fig. 2. Comparison of pruritus characteristics in patients with systemic sclerosis (SSc) according to their autoimmune status. (A) Current pruritus intensity, on average, best time and worse time as determined, quantitative analysis using a scale from 0 to 10. (B) Pruritus intensity per day, qualitative analysis. (C) Pruritus duration per day. (D) Pruritus location according to the sclerotic area. When significant p < 0.05 are indicated. ACA: anti-centromere antibodies.
Finally, as we have observed differences for pruritus characteristics (duration/day, intensity, and location) between ACA+ and ACA– SSc patients, we further suspected different impacts on their QoL. To answer this question, 41 parameters evaluating the impact of pruritus on sleep, social interactions, work, leisure and psychological consequences were tested (Table SI). For the parameter “I spend more money on dermocosmetics”, a higher impact of pruritus was reported in the ACA– SSc subgroup (p = 0.05). With regard to the 22 parameters of the Itchy-QoL scale score (23), there is a trend towards lower values in the ACA+ SSc subgroup. In contrast, similar values were observed in both groups with regards to the impact of pruritus on activities of daily living.
The pathophysiology of pruritus in patients with SSc is unknown. A better understanding of the mechanisms is particularly important, since treatment of pruritus in SSc is challenging. The management of pruritus is poorly codified, consisting of antihistaminic lubrication of the skin, reduced bathing to prevent dryness of the skin, massage and exercise (1). The current study, conducted in 56 patients with SSc, found differences regarding pruritus characteristics when patients were subdivided according to the presence of ACA. Among patients with ACA+ presenting a limited SSc, the pruritus was characterized by a lower intensity per day, localization mainly restricted to non-sclerotic area, and a trend to present improvement in QoL parameters. Another argument to support the concept that pruritus and SSc processes are linked is related to the fact that both events appeared concomitantly in most cases; however, this study did not find a link between pruritus and a particular immunological profile in SSc.
Several arguments support a neuropathic component in the pathophysiology of pruritus in SSc. This assertion is further supported by our previous clinical observations in SSc, that pruritus is associated with sensory symptoms that predominate in the extremities and non-sclerotic areas (7). A possible explanation for this is that compression of small nerve fibres by thickened and/or dense collagen contributes to the neuropathic component (25, 26). In addition, an inflammatory and immunological component of neuropathic pruritus had also been adduced by regeneration of C-fibers after destruction by collagen deposition and increasing sensitization of itch fibres by inflammatory mediators (27). If a neuropathic component of pruritus is confirmed in SSc by further research, this would open interesting therapeutic propositions based on the utilization of low doses of naltrexone (28), antidepressant treatments (29), gabapentin or pregabalin (30), and JAK inhibitors, since their efficiency in treating chronic pruritus has been demonstrated recently (31). Interestingly, blocking JAK1/JAK-2 is further suspected to have an antifibrotic effect in cultured fibroblasts and experimental dermal and pulmonary fibrosis models. Research into small fibre neuropathy and, in particular, non-histamine dependent C-fibers will be necessary to support the neuropathic component of pruritus in SSc and, more particularly, in those with ACA. Qualitative and/or quantitative abnormalities in the synthesis of extracellular matrix components or even microvascular abnormalities should also be considered in the pathophysiology of pruritus.
The predominance of pruritus in sclerotic areas in the ACA– SSc subgroup could be explained by a preponderant neuropathic component of pruritus related to the compression of small cutaneous nerve fibres (polymodal C-fibers) in this subgroup. This may be related to a higher degree of fibrosis in the affected skin areas in patients in this group. Another hypothesis would be a higher level of IL-4, a cytokine known both for its pro-pruritogenic and pro-fibrotic properties, in the cutaneous zones of fibrosis in this ACA– subgroup (32).
The higher rate of pruritus outside the areas of sclerosis in the ACA+ group could be explained by factors such as: (i) a skin surface affected by less extensive fibrosis; (ii) a circulating rate or cutaneous release of pruritogenic cytokines (in particular IL-31). This latter hypothesis would require a prospective study, considering the cutaneous and circulating levels of pruritogenic cytokines on and off the fibrosis zones in patients with cutaneous scleroderma, taking into account their autoimmune status.
From the genetic point of view, various studies have determined that several genetic mutations, such as IL-31, filaggrin (FLG), kinesin family member 3A (KIF3A), and opioid receptor contributed to pruritus (33), and that genetic mutations are involved in SSc, with the particularity that specific genetic profiles are associated with different clinical subtypes of SSc (5). Indeed, genome-wide association studies (GWAS) have highlighted strong associations in ACA+ patients with B-lymphocytes kinase gene (BLK), tumour necrosis factor super family member 4 (TNFSF4) and neurogenic locus notch homolog 4 (NOTCH4) variants, while for ACA– patients such associations were reported with interleukin 1 receptor associated kinase 1 (IRAK1) and toll-like receptor 2 (TLR2) variants (34). Future studies are also needed to test associations between genetic variants and clinical parameters, including pruritus, among SSc subtypes. If true, the genetic hypothesis further supports that therapeutic treatments for pruritus have to be adapted according to the clinical and immunological subgroups of SSc.
Among the different pruritogen mediators, both lyso-phosphatidic acid (LPA) and vitamin D are dysregulated in SSc and they are suspected of contributing to the pathogenesis of the disease by promoting dermal fibrosis and calcinosis, respectively (35). First, an elevated level of serum LPA is reported in SSc, and blocking the enzyme responsible for its synthesis, autotaxin (ATX), using the novel PTX inhibitor PAT-048, prevents dermal fibrosis (36). Future studies are needed to test the effects of this inhibitor on pruritus, as the intradermal injection of LPA induces scratching responses in mice by activation of LPA1 receptor and opioid µ receptor (37). LPA receptor activation promotes the hyperpermeability of venules and the pathological uptake of immune cells, aggravating pruritus. Similar to LPA, ATX activity is correlated with pruritus severity (38). Secondly, the ACA+ SSc subgroup is suspected to be more responsive to vitamin D supplementation, as the presence of ACA correlates with the normalization of vitamin D levels after supplementation (39). This is important, as an inverse relationship between serum levels of vitamin D and SCORAD index has been shown in atopic dermatitis (AD) (40). To our knowledge, LPA, vitamin D and other pruritogenic mediators of interest, such as IL-31, have not been associated with pruritus. In addition, the effects of vitamin D supplementation on pruritus in SSc and SSc subgroups are not known.
Toll-like receptors (TLR), germline-encoded pattern recognition receptors, are new players identified in the processing of pruritus by increasing the excitability of primary sensory neurones (41). The direct link between TLR activation and pruritus is further supported by the description of TLR3, TLR4 and TLR7 in a subset of pruriceptive/nociceptive neurones in the dorsal root and trigeminal ganglion (42). However, TLR are also involved in SSc pathophysiology. Subcutaneous injections of TLR ligands into the skin of SSc induce a significant inflammatory reaction, resulting in SSc skin changes (35, 43). On the other hand, TLR expression is increased in fibroblasts from patients with SSc (35, 44). In addition, immune complexes from the ACA– SSc subgroup contain RNA that could bind intracellular TLR7 (45). Thus, the development of new blockers for Myd88 at the crossroads of the TLR pathway opens new opportunities to treat SSc and pruritus.
Cytokines are also emerging as important mediators in pruritus, as small diameter neurones NP1, NP2 and NP3, predicted to mediate pruritus, have an increased expression of IL-4-RA and IL-13-RA1 compared with other families of nociceptive and mechanoreceptive neurones (18). Such an observation is important, since SSc is defined as a Th2-predominant disease (46) and could explain how type 2 cytokines, such as IL-4, sensitize sensory neurones to many pruritogens without being pruritogenic themselves. In addition, this theory provides an explanation for the observation that chronic pruritus can manifest in both the affected skin areas of SSc and the non-affected skin areas. It has been demonstrated that type 2 cytokines directly activate both mice and human sensory neurones via TRP channel-dependent calcium influx (18). In fact, IL-4 enhances neuronal responsiveness to multiple types of pruritogens. A recent study has shown that human dorsal root ganglia express IL-4-RA, IL-13-RA1 and IL-31-RA (18). Thus, exploring the cytokine profiles of these patients, including IL-4 and IL-31, at the local and peripheral levels could also reveal the pathophysiology of pruritus in the SSc and SSc subgroups.
This study has several limitations. The statistical power is low, due to the small population size. It has a long period of recruitment, leading to a biased selection with omission of those with severe diseases (55/137 deaths). The collection of biological data was retrospective, and there are selective memory biases linked to the questionnaire. A prospective and replicative cohort is now needed in order to validate such observations.
In conclusion, this study has contributed to unmasking different semiological characteristics of pruritus in SSc and has provided arguments to suggest differences according to the autoimmune subtype of SSc. Future studies are needed to better characterize mechanisms controlling pruritus in the different subtypes of SSc in order to better manage this disabling symptom, which can have a significant impact on patients’ QoL, independent of the other disabling manifestations of SSc.
The authors would like to thank Dr Wesley H. Brooks (University of South Florida, FL, USA) for editorial assistance and to Simone Forest and Genevieve Michel for secretarial assistance. Brest University Hospital supported this study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize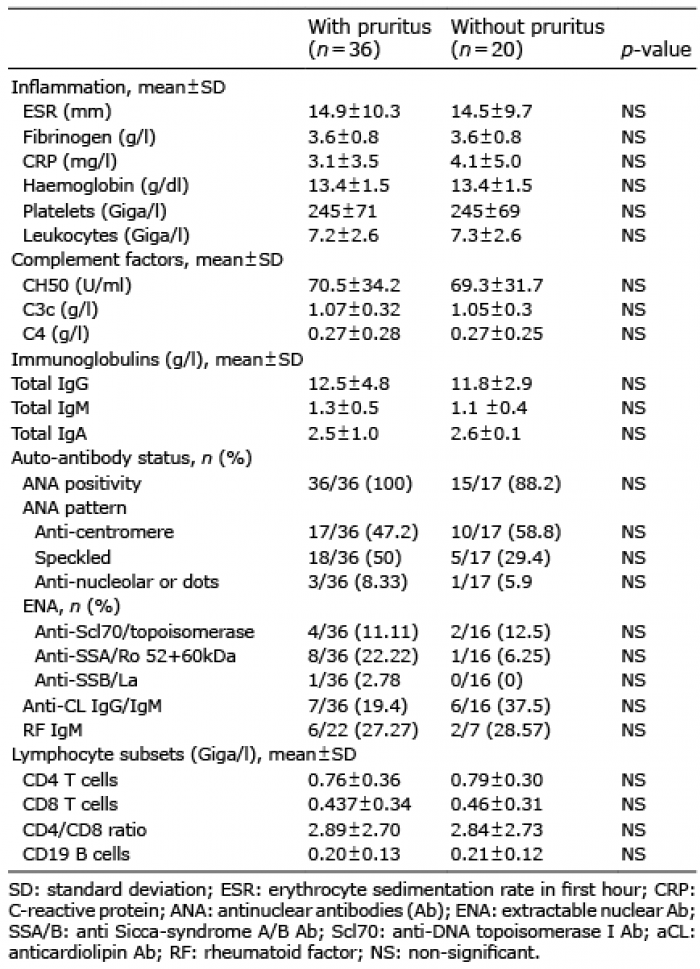 Click to show fullsize
Click to show fullsize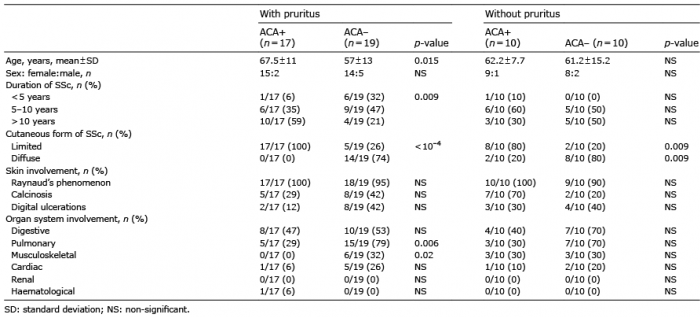 Click to show fullsize
Click to show fullsize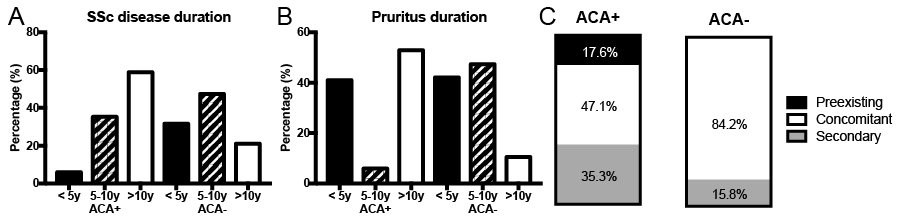 Click to show fullsize
Click to show fullsize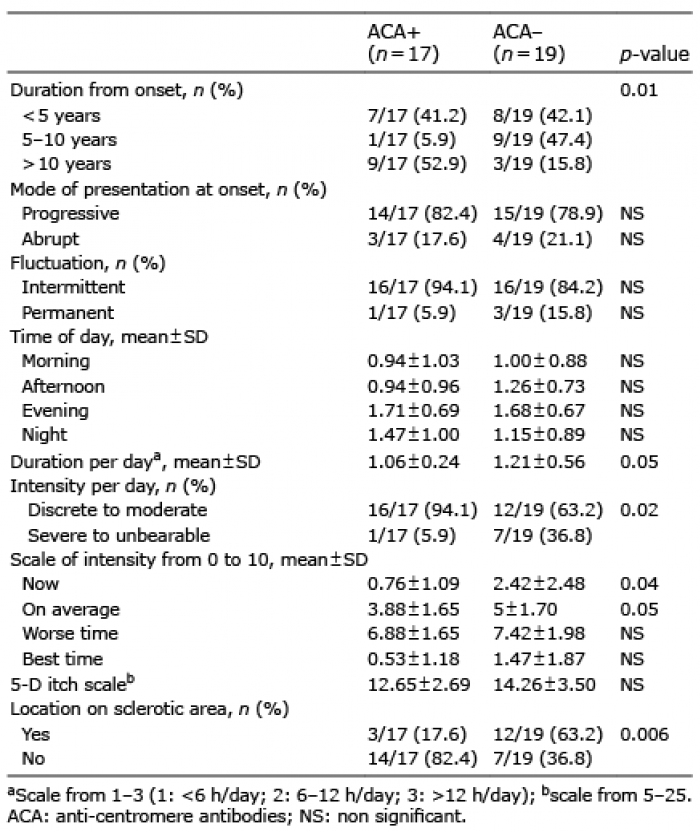 Click to show fullsize
Click to show fullsize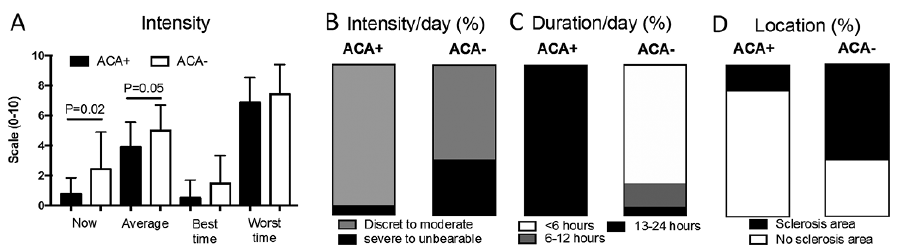 Click to show fullsize
Click to show fullsize