


Center for Blistering Diseases, Department of Dermatology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands
Mechanobullous epidermolysis bullosa acquisita (mEBA) can have a clinical presentation that is very similar to other blistering diseases, such as porphyria cutanea tarda (PCT) and pseudoporphyria. Direct immunofluorescence is an important feature in the diagnosis of mEBA, although features that overlap with PCT and pseudoporphyria have been reported. This retrospective observational study investigated whether direct immunofluorescence can discriminate mEBA from PCT and pseudoporphyria. Biopsies of 13 patients with mEBA, 10 with PCT and 10 with pseudoporphyria were included. In 7 cases of PCT and 4 of pseudopor-phyria, direct immunofluorescence showed a pattern at the dermal–epidermal junction that appeared similar to the u-serrated pattern in mEBA. Vessel wall depositions were observed in all 3 diseases, but were more frequent and more intense in PCT and pseudoporphyria than in mEBA. Careful examination of direct immunofluorescence of mEBA vs. PCT and pseudoporphyria revealed different staining patterns, although overlapping features were present. Therefore, integrating all clinical and laboratory data is essential to differentiate between mEBA, PCT and pseudoporphyria.
Key words: mechanobullous epidermolysis bullosa acquisita; porphyria cutanea tarda; pseudoporphyria; direct immunofluorescence microscopy.
Accepted Aug 29, 2018; Epub ahead of print Sep 3, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Gilles F. H. Diercks, Center for Blistering Diseases, Department of Dermatology, University Medical Center Groningen, Hanzeplein 1, NL-9700 RB Groningen, The Netherlands. E-mail: g.f.h.diercks@umcg.nl
Mechanobullous epidermolysis bullosa acquisita, porphyria cutanea tarda and pseudoporphyria are mechanobullous diseases that have many clinical similarities, but have a different pathogenesis and need different treatment. It is therefore important to separate these entities. We performed a retrospective observational study to compare clinical and laboratory data, in particular direct immunofluorescence, of these patient groups in order find discriminatory features. Careful examination of these data revealed (subtle) differences, although many overlapping features are present. Therefore, integrating all clinical and laboratory data is essential to differentiate between mechanobullous epidermolysis bullosa acquisita, porphyria cutanea tarda and pseudoporphyria.
Epidermolysis bullosa acquisita (EBA) is a rare subepidermal autoimmune bullous disease. The classic mechanobullous subtype (mEBA) may mimic porphyria cutanea tarda (PCT) and pseudoporphyria. Clinically these diseases are characterized by acral blisters that heal with atrophic scarring and milia, whereas histological examination shows cell-poor subepidermal blistering in all 3 entities. Although higher sensitivities have been reported (1, 2), in our experience serology has a sensitivity of only 40% for salt-split skin (SSS) and 45% for NC1/NC2 type VII collagen enzyme-linked immunoassay (ELISA) in patients with EBA (3), serration pattern analysis by direct immunofluorescence microscopy (DIF) is considered of the utmost importance for diagnosis. In EBA in vivo depositions of immunoglobulins at the epidermal basement membrane zone (BMZ) are usually in a u-serrated linear pattern (4), whereas in PCT and pseudoporphyria homogenous depositions of fibrinogen, complement and immunoglobulins are found in the BMZ of epidermis and vessel walls (5, 6). However, in daily practice mEBA, PCT and pseudoporphyria can show very similar epidermal BMZ staining patterns. DIF patterns of mEBA, PCT and pseudoporphyria have never been compared systematically. The aim of this study is to re-evaluate clinical information and histopathology of confirmed mEBA, PCT and pseudoporphyria cases and to repeat DIF on archived frozen biopsies in order to re-examine features that may differentiate between these diseases.
Patients were selected from the biobank of the Center for Blistering Diseases of the University Medical Center Groningen (UMCG) for the period 1990 to 2016. Inclusion criteria for mEBA were: (i) mechanobullous blisters, (ii) a u-serrated pattern of linear immunodeposits of IgG at the epidermal BMZ by DIF of skin tissue, and/or (iii) dermal staining on SSS substrate and/or autoantibodies to type VII collagen established by NC1/NC2 type VII collagen ELISA and/or reactivity to the 290-kDa band by immunoblot on dermal extract. The mEBA patients have been reported previously (7), but do not represent our total mEBA population, since only those patients with positive serological results were included in this study. Inclusion criteria for PCT were: (i) blisters on sun-exposed skin, with (ii) elevated porphyrin levels in urine and/or serum. Inclusion criteria for pseudoporphyria were: (i) blisters on sun-exposed skin, with (ii) no elevation of porphyrin levels in urine and/or serum, and (iii) remission of cutaneous disease after cessation of the causative drug and/or sun exposure. At the time biopsies were obtained, all patients consented to the use of material for further diagnostic or research purposes in the future. In this retrospective study, no approval by the ethics committee in the Netherlands was required according to national regulations.
The frozen biopsies were cut to 4-µm thick sections and stained for DIF with IgG, IgA, IgM, fibrinogen and C3c, as described previously (4). The sections were examined with a Leica DMRA fluorescence light microscope (Leica, Wetzlar, Germany). DIF staining intensities were graded from 1+ to 4+ by 2 blinded observers (HdG and GD). Fluorescence photographs were taken of the epidermal BMZ and the dermal blood vessels of each of the slides using a Leica DFC350FX camera. Leica Application Suite software (version 3.8.0) and Adobe Photoshop CS6 (version 13.0.1 ×32) were used for further image processing. Fluorescence overlay antigen mapping (FOAM) was used to map in vivo bound IgG at the epidermal BMZ with type VII collagen. This was performed in 2 cases of mEBA, 3 cases of PCT and one case of pseudoporphyria, which showed an IgG serration pattern at the epidermal BMZ very similar to the u-serration pattern of mEBA. The mapping procedure included 3 successive immunostaining steps, with incubation at room temperature for 30 min and rinsing with PBS for 15 min between each step. The first step involved adding mouse anti-human type VII collagen IgG (LH7.2) to the frozen sections. Secondly, highly cross-absorbed Alexa Fluor® 568 goat anti-mouse IgG (Molecular Probes Europe, Leiden, The Netherlands) was added. The third step involved adding Fc-specific FITC-conjugated goat F(ab’)2 anti-human IgG (Protos Immunoresearch, USA). Lastly, bisbenzimide (Hoechst 33258) was placed on the slides and incubated for 5–10 min to provide nuclear staining. Afterwards the slides were washed with PBS for 15 min and a coverslip with a drop of SlowFade® was placed on each section.
All clinical information and photodocumentation for patients was collected from the UMCG electronic patient file system. When available, histopathological slides of haematoxylin-eosin- (H&E) and periodic acid-Schiff- (PAS) stained paraffin sections were examined by light microscopy. Other previously performed laboratory test results were retrieved from our database: indirect immunofluorescence with SSS, immunoblot analysis on reactivity to the 290-kDa antigen on human dermal extract, and type VII collagen ELISA. In mEBA, results from SSS showed dermal staining in 10 cases (77%). Immunoblot reactivity to the 290-kDa band was present in 6 cases (46%), and ELISA to type VII collagen was positive in 8 cases (67%).
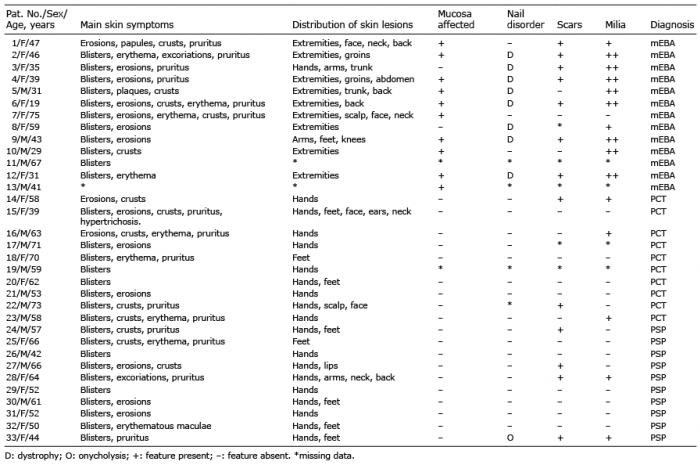
The patients’ clinical characteristics are shown in Table I. A total of 13 patients with mEBA were included. In all but 1 patient, the diagnosis of mEBA was confirmed by serology. In patient 1 there was a very clear u-serrated pattern by DIF, but negative serology; however, antigen mapping with type VII collagen confirmed mEBA as the diagnosis. The median age at diagnosis was 41 years (range 19–75 years) of mEBA patients was younger than PCT (60.5; range 39–73 years) and pseudoporphyria patients (54.5; range 42–66 years). In all mEBA patients the skin manifestations were not limited to the hands and feet. In 7 mEBA patients erosions healed with scars, and milia were present in 10 cases (Fig. 1A and C). For both PCT and pseudoporphyria, the skin manifestations were limited to the hands and/or feet in 16 out of 20 patients, with scarring and milia occurring less frequently and less severely than in mEBA (Fig. 1B and D). In mEBA, mucosal involvement was present in 10 cases (Fig. 1F). In all of these cases the oral mucosa was involved, in one case there was also genital, nasal and ocular involvement. In PCT and pseudoporphyria, none of the patients had mucosal involvement. Nail dystrophy was present in 8 mEBA cases, in 4 of those cases 1 or more nails were completely absent (Fig. 1E). In PCT and pseudoporphyria nail dystrophy was not present. In patient 33 there was a nail abnormality characterized by mild distal onycholysis of the toenails of the halluces, but it is uncertain whether this was related to the pseudoporphyria.
Table I. Clinical characteristics of 13 patients with mechanobullous epidermolysis bullosa acquisita (mEBA), 10 with porphyria cutanea tarda (PCT) and 10 with pseudoporphyria (PSP)
Fig. 1. Clinical manifestations of epidermolysis bullosa acquisita (EBA), porphyria cutanea tarda (PCT) and pseudoporphyria. (A) Blister on the arm of patient 6 (EBA). (B) Tense bulla on finger and excoriations and reddish-brown maculae with a few milia on the dorsal side of the hand of patient 28 (pseudoporphyria). (C) Pink erythematous papules with milia on the dorsal side of the hand of patient 5 (MB-EBA). (D) Erythematous plaques with milia and several rhagades on the dorsal side of the hand of patient 14 (PCT). (E) Nail dystrophy in patient 12 (EBA). (F) Oral lesion in patient 2 (EBA).
All immunological findings are shown in Table II. In mEBA, DIF examination showed a linear/u-serrated pattern of IgG depositions at the epidermal BMZ in 12 cases (Fig. 2a), in one case the pattern was undetermined. Coarse clumps of IgG depositions at the epidermal BMZ were observed in 3 cases (23%, Fig. 2b). In PCT and pseudoporphyria, the depositions at the epidermal BMZ were mostly homogenous, but there was a variation of patterns. In 7 PCT and 4 pseudoporphyria cases, parts of the depositions at the epidermal BMZ appeared very similar to a u- or n-serrated pattern (Fig. 2c–e). Mostly, they were not as intense and not as finely delineated, although in some instances it was difficult to discern between mEBA and (pseudo)porphyria. In these cases the depositions were called “pseudo-serrated”. Vessel wall depositions were present in 4 mEBA cases, although less intense than the depositions at the epidermal BMZ. In PCT and pseudoporphyria, vessel wall staining was present in all patients but 1 (Fig. 2c). Patient 21 only showed depositions at the epidermal BMZ. Mostly the depositions in the vessel walls were of similar intensity or more intense than the depositions at the epidermal BMZ (Fig. 2f). Compared with mEBA, vessel wall depositions in PCT and pseudoporphyria showed more intense staining.
FOAM mapping in vivo bound IgG with type VII collagen showed in PCT and pseudoporphyria that the pseudo-u-serrated parts of IgG depositions at the epidermal BMZ had an almost complete overlap with type VII collagen, although some depositions appeared to be below and above type VII collagen (Fig. 2g–i). As expected, in mEBA there was a complete overlap of IgG with type VII collagen (not shown).
Table II. Immunopathological characteristics
Fig. 2. Direct immunofluorescence microscopy. (a) u-serrated depositions of immunoglobulin IgG (3+) at the epidermal basement membrane zone (BMZ) in patient 1 (epidermolysis bullosa acquisita; EBA). Insert shows the u-serrated pattern in detail (b), “coarse clumps” depositions of IgG (3+) at the epidermal BMZ in patient 13 (EBA). (c) Partly pseudo-u-, partly pseudo-n-serrated (arrow) depositions of IgG (+) at the epidermal BMZ in patient 21 (porphyria cutanea tarda; PCT). Insert shows the pseudo-u-serrated pattern in detail. (d) Pseudo-u-serrated depositions at the epidermal BMZ (3+) and homogenous depositions of IgG in vessel walls (3+) in patient 29 (pseudoporphyria). (e) Homogenous depositions (3+) at the epidermal BMZ with homogenous depositions of IgG in vessel walls (4+) (arrow) in patient 20 (PCT). (f) Classic intense depositions of IgG (4+) in vessel walls and homogenous depositions (3+) at the epidermal BMZ in patient 14 (PCT). Fluorescent overlay antigen mapping of a porphyria patient. (g) IgG depositions showing a pseudo-u-serrated pattern at the epidermal BMZ in green. (h) Staining of collagen type VII in red. (i) Overlay of IgG and collagen type VII, showing IgG and collagen type VII, partially overlapping in orange. Bars: (a–e, g–i) 20 μm, (f) 150 μm.
Histopathological sections were available for 2 patients with mEBA, 3 with PCT and 8 with pseudoporphyria. All showed cell-poor subepidermal blisters (Fig. 3). Festooning was present in all cases of PCT and 3 cases of pseudoporphyria (38%), as well as in one case of EBA (50%). The PAS- and collagen IV-stains showed thickening of vessel walls in all cases of PCT and 5 cases of pseudoporphyria (63%), but in none of the cases of mEBA. Caterpillar bodies were observed in one case of PCT (33%) and one of pseudoporphyria (13%).
Fig. 3. Histological findings in porphyria cutanea tarda (PCT). Periodic acid-Schiff (PAS)-stain shows: (A) festooning of the dermal papillae (arrows) and thickened basement membrane zone (BMZ) of vessel walls (arrowheads) in patient 15 (20×). (B) Caterpillar bodies in the epidermis of patient 23 (arrowheads) (40×).
Table III summarizes the differences and similarities of mEBA, PCT and pseudoporphyria that can be derived from this study.
Table III. Comparison of mechanobullous epidermolysis bullosa acquisita (mEBA) vs. porphyria cutanea tarda (PCT) and pseudoporphyria
This study comparing mEBA, PCT and pseudopor-phyria shows that, at first sight, these bullous diseases can have similar immunofluorescence staining patterns, although, on close examination, differences can be revealed.
DIF showed a u-serrated pattern of IgG and complement depositions at the epidermal BMZ in 92% of the cases of mEBA in the current study. In PCT and pseudoporphyria, mainly homogenous depositions of IgG were seen at the epidermal BMZ. However, in a substantial number of PCT and pseudoporphyria cases a pseudo-serrated pattern was observed in a section of the slide. Comparing these pseudo-serrated depositions to the u-serrated depositions seen in mEBA, it varied from a very weak to a strong resemblance. However, it can be said that in (pseudo)porphyria the depositions at the epidermal BMZ were less intense and less finely delineated compared with mEBA. Little research has been performed so far in this area, but a u-serrated pattern in PCT has been observed previously (8), underscoring the potential difficulty of separating EBA from (pseudo)porphyria with DIF.
FOAM analysis showed that, similar to mEBA, in PCT and pseudoporphyria the IgG depositions overlapped with type VII collagen, explaining that a serration pattern similar to the u-serration in mEBA can be found. This suggests that photo-active substances, such as por-phyrins or active drug metabolites and formed immune complexes, are deposited at the same height as collagen VII. In 2 cases of PCT in our group, not only a pseudo-u-serrated pattern was seen, but also focally a pseudo-n-serrated pattern. Vodegel et al. (4) studied 157 biopsies from patients with subepidermal autoimmune bullous diseases and found that the 2 serration patterns did not coexist. Therefore, if both patterns are seen in one biopsy this should raise the suspicion of (pseudo)porphyria.
Deposition of immunoglobulins in the BMZ of vessel walls is a feature frequently described in PCT and pseudoporphyria. mEBA, PCT and pseudoporphyria all showed some degree of vessel wall staining in the papillary dermis, although in PCT and pseudoporphyria vessel wall depositions were found in almost all cases, whereas in mEBA this was present in approximately one-third of cases. Moreover, the staining of immunoglobulins in the vessel walls was more intense in PCT and pseudoporphyria than in mEBA. In this respect, Gupta et al. (9) stated that PCT can mimic mEBA clinically, but that DIF depositions around the vessel walls distinguishes mEBA from PCT. A new finding in our study is that vessel wall depositions can occur in all 3 diseases, but the intensity of the staining is important to differentiate mEBA from (pseudo)porphyria.
However, one of the cases of PCT in our study showed deposition of immunoglobulins at the epidermal BMZ without vessel wall depositions. This was also observed in a previous study of DIF in a total of 28 patients with PCT that took biopsies in 3 phases: before treatment, during clinical remission and during biochemical remission (5). Supporting our results, of the 23 biopsies that were taken before treatment, DIF showed homogenous and intense depositions at the epidermal BMZ and in vessel walls. However, in 2 cases of PCT before treatment, they observed depositions of IgG at the epidermal BMZ without depositions in the vessel walls. In one of those patients a second biopsy was taken during clinical remission, in which DIF showed depositions of immunoglobulins in the vessel walls while the depositions at the epidermal BMZ were no longer present. This suggests that the biopsy of our patient was probably taken at a time-point in the active phase when there was not yet any vessel wall deposition.
Besides immunofluorescence this study also shows that, on dermatological examination, differences between mEBA and (pseudo)porphyria could be observed. Mucous membrane involvement and nail dystrophy were present only in mEBA. Mucosal involvement is said to be present frequently in mEBA. In this respect, Iranzo et al. (10) found mucous membrane involvement in 3 out of 5 mEBA patients. In contrast, mucosal involvement in PCT and pseudoporphyria is not a dominant feature, although it has rarely been described (11). Similar to our study, nail dystrophy is reported to be common in mEBA (9, 12). Nail dystrophy is not known to occur in (pseudo)porphyria, although another nail abnormality, photo-onycholysis, has been described (13, 14). This, however, was not present in any of the 20 patients with (pseudo)porphyria in the current study. A third distinctive clinical feature was the more extensive presence of milia and scarring in the patients with mEBA.
Since histopathological biopsies were not present for all patients, results have to be interpreted with care. However, we could discern several histological features that are specific for (pseudo)porphyria. In the first place, thickened walls of papillary blood vessels were found in all PCT cases and in almost all pseudoporphyria cases, whereas this was not present in either of the 2 cases of mEBA. Thickened blood vessel walls have been described as a common feature in PCT and pseudoporphyria (5, 12, 15, 16).
A second distinctive feature were so-called caterpillar bodies (Fig. 2), which were present in one case of PCT and 1 of pseudoporphyria, but in none of the cases of mEBA. It is known that these eosinophilic, linear-arranged segmented bodies found in the blister roof are seen mostly in the porphyrias (17). Similar to our study, Egbert et al. (18) found caterpillar bodies, not only in PCT, but in pseudoporphyria too.
Festooning is recognized as a classic feature of PCT and pseudoporphyria (13, 16, 17). Indeed, festooning was found in all our cases of PCT and 38% of cases of pseudoporphyria. Although it has been reported that mEBA lacks festooning (19), festooning was observed in one of our patients with mEBA. This supports earlier findings, showing festooning in mEBA in 2 out of 4 reviewed cases of mEBA (17).
A limitation of the current study is that, due to its retrospective nature, not all serological tests were performed in the PCT and pseudoporphyria groups. Although, serology on SSS was performed in a majority of cases (and was negative in all cases), we cannot completely rule out concomitant mEBA. Conversely, in the mEBA patients porphyrins were not measured, thus PCT is also not completely ruled out in these patients.
The results of the current study support the general conception that mEBA, PCT and pseudoporphyria can have very similar clinical, histopathological and DIF features. Given the fact that these diseases are so alike, the first step in the diagnostic work-up is to order urine analysis for porphyrins. DIF has substantial value in the diagnostic work-up in order to differentiate EBA from PCT and pseudoporphyria, but on its own it cannot be regarded as the gold standard. In a patient with a mechanobullous skin disease, it is essential to integrate all clinical and laboratory data in order to differentiate between mEBA, PCT and pseudoporphyria.
The authors would like to thank Gonnie Meijer and Marije van der Molen for laboratory assistance.


 Click to show fullsize
Click to show fullsize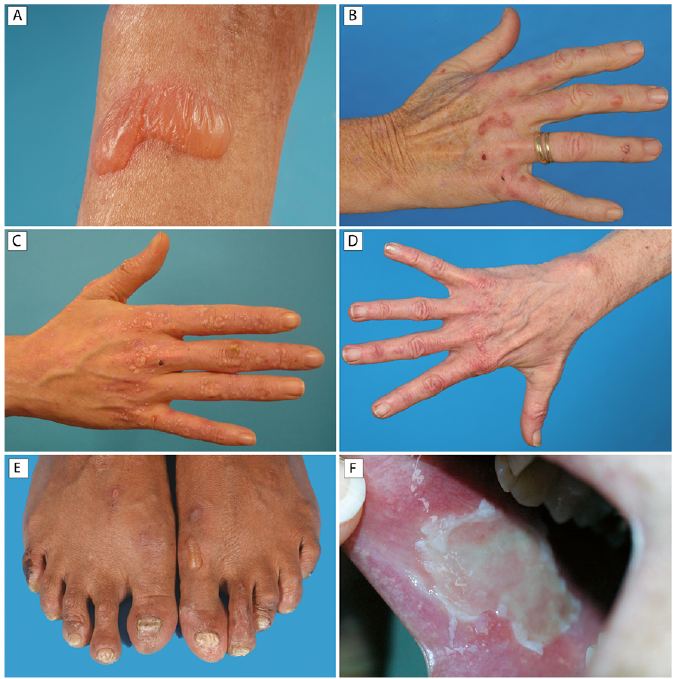 Click to show fullsize
Click to show fullsize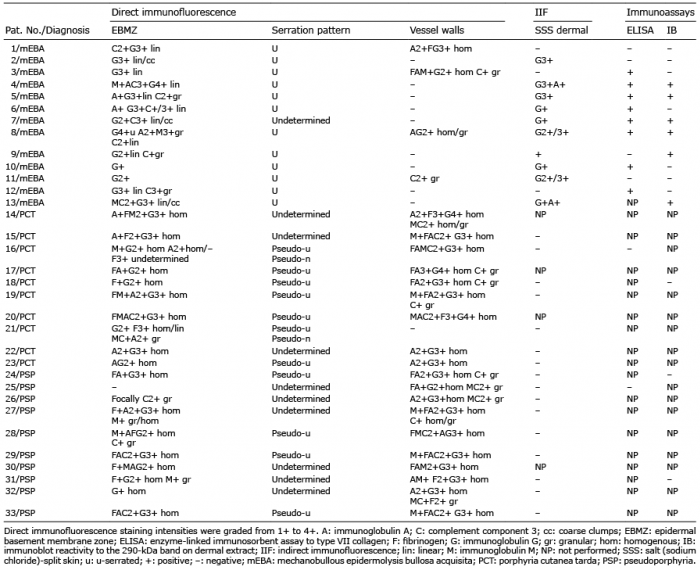 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize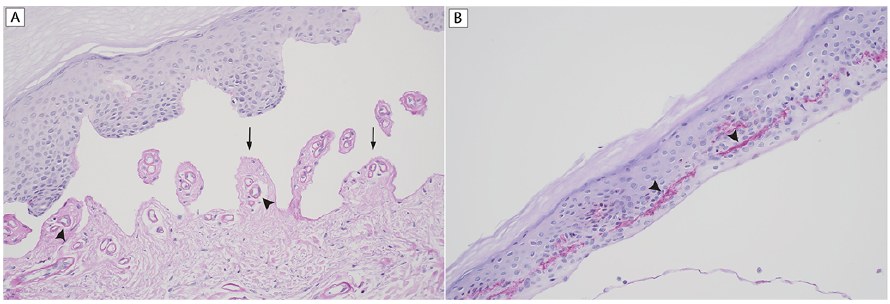 Click to show fullsize
Click to show fullsize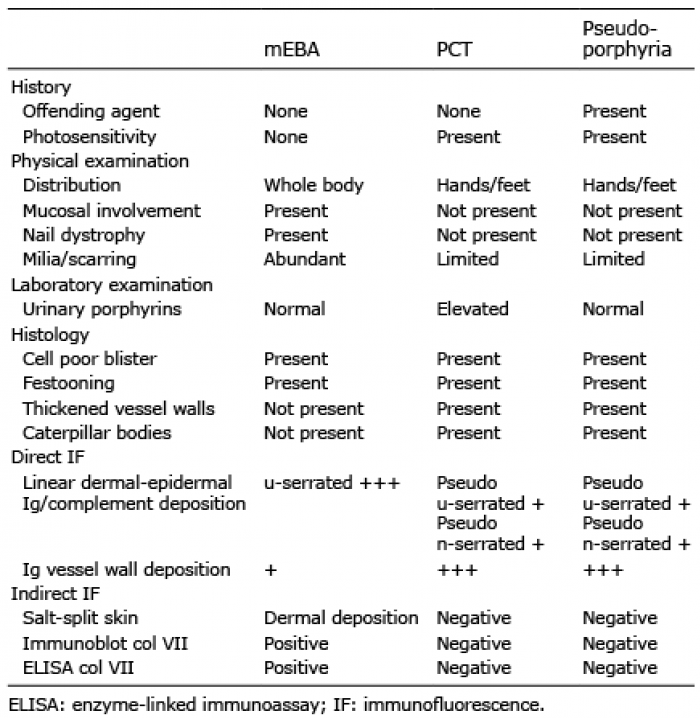 Click to show fullsize
Click to show fullsize