


1Department of Rheumatology, 4Clinical Pharmacology and 5Department of Dermatology, Hospital Universitari Parc Taulí, Sabadell, 2Department of Rheumatology, Parc de Salut Mar, 3Department of Dermatology, Parc de Salut Mar, Universitat Autònoma de Barcelona/Universitat Pompeu Fabra, Barcelona, Spain
?Dr Lisbona died just before completion of the study.
This cross-sectional study evaluated the usefulness of an ultrasound technique in assessment of nail changes in 35 patients with psoriatic onychopathy and 25 with nail dystrophy secondary to onychomycosis. All patients underwent 3 examinations: a complete clinical assessment; a nail ultrasound study; and fungal culture. Nails of patients with psoriatic onychopathy presented a thinner nail plate and nail bed, measured by ultrasound, than did those with onychomycosis. The percentage of patients with a power Doppler signal ≥2 at nail bed was significantly higher in psoriatic onychopathy than in onychomycosis, and structural bone lesions were more frequent in psoriatic onychopathy than in onychomycosis. These results suggest that the presence of structural damage and high-power Doppler signal are the main ultrasound findings supporting a diagnosis of psoriatic onychopathy.
Key words: ultrasound; nail; psoriatic onychopathy; onychomycosis.
Accepted Oct 3, 2018; Epub ahead of print Oct 3, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Fernando Gallardo, Department of Dermatology, Parc de Salut Mar, Universitat Autònoma de Barcelona/Universitat Pompeu Fabra, ES-08003 Barcelona, Spain. E-mail: fgallardo.fg@gmail.com
Ultrasound is an emerging, non-invasive, inexpensive, imaging technique with proven evidence for use in the assessment of different skin disorders. The aim of this study was to differentiate nail psoriasis from onychomycosis using an ultrasound technique, since clinical differentiation of these conditions is challenging, especially if psoriasis presents with nail disease alone. The long-term therapy and prognosis for these disorders are different, therefore early and adequate diagnosis is essential. Presence of structural bone damage and a high-power Doppler signal were the main observed ultrasonographic findings supporting a diagnosis of nail psoriasis and suggesting an association with psoriatic arthritis.
Psoriatic arthritis (PsA) is a heterogeneous chronic inflammatory disease with a wide clinical spectrum and variable course. Early diagnosis and treatment of PsA could contribute to the prevention of clinical and radiological progression and functional deterioration (1, 2).
Nail involvement is common in patients with psoriasis. Nails are affected in 15–50% of patients with psoriasis, with the lifetime incidence of nail involvement being approximately 80% (3). Although psoriatic onychopathy (PsO) is diagnosed solely on the basis of clinical signs, it is considered a major clinical marker for the presence or development of PsA. Moreover, PsO is often the only psoriatic finding at the time of PsA diagnosis in cases with no other cutaneous lesions of psoriasis.
Eight features of PsO have been identified for the Nail Psoriasis Severity Index (NAPSI) score: 4 involve the nail matrix (pitting, leukonychia, red spots in the lunula, and nail plate crumbling) and 4 the nail bed (onycholysis, splinter haemorrhages, subungueal hyperkeratosis, and oil spot/salmon patch). The NAPSI (4) is an objective and reproducible tool for estimating the severity of PsO, intended as a good measurement of the efficacy of therapeutic interventions.
Ultrasound (US) has proven a useful, non-invasive and inexpensive imaging technique for screening superficial tissues, such as the nails (5–7). Substantial evidence for the role of US in the assessment of onychopathy in PsA has been published (8, 9). However, to our knowledge, no previous studies have analysed the capacity of this imaging technique to help clinicians differentiate PsO from other nail changes. Onychomycosis (OM) affects 3–4% of the population, with prevalence increasing with age (10, 11). Clinical differentiation between PsO and OM is challenging, especially when nail disease alone is present. PsO and OM have different clinical and prognostic implications and require different long-term therapy with potential side-effects, it is essential to ensure both an early and adequate diagnosis (12).
The aims of this study are to evaluate the usefulness of US in the assessment of PsO, and to differentiate PsO US findings from those found in OM.
This was a cross-sectional study in which consecutive psoriatic patients with nail involvement (with or without PsA according to Classification Criteria for Psoriatic Arthritis (CASPAR) classification criteria) (13) and patients with suspected OM attending rheumatology and dermatology out-patient clinics in Barcelona and Sabadell (Spain) for 1 year, were invited to participate. Ethical approval was obtained from the local ethics committee, and patients provided written consent.
All included patients underwent 3 examinations performed by different clinicians: a complete clinical assessment; a nail US study; and a fungal culture. Patients with nail injuries, current oral or topic antifungal therapy or those with concomitant PsO and positive fungal culture were excluded from the study. Only those patients with positive confirmed dermato-phyte cultures and no past medical (personal and familial) history of psoriasis were included in the OM control group. No systemic or biologic treatments for PsO were prescribed at the time of US examination.
Subjects were interviewed and examined by 4 experienced dermatologists for the diagnosis of PsO or OM. Age, sex, duration of nail disease, severity of nail involvement, treatments, a count of finger and toe nails affected by psoriasis, and the presence of pitting, onycholysis, salmon patches, subungueal hyperkeratosis, thickening of the nail plate and splinter haemorrhages were recorded.
For estimation of the severity of PsO, NAPSI index evaluation was performed. NAPSI is a standard method for the evaluation of PsO severity, but an approximation to quantification using the NAPSI index was also applied to OM changes in order to compare the severity of nail disease in these disorders. Each nail was divided into 4 quadrants. Each quadrant was evaluated for the presence of any manifestation of psoriasis in the nail matrix or nail bed. The lesion(s) of nail matrix and nail bed were given a score of 1 in each quadrant, yielding a matrix score of 0–4 and a nail bed score of 0–4 per nail, with a total maximum score of 8 and a minimum score of 0 per nail (14).
US nail assessment was performed by 3 rheumatologists who used US imaging on a regular basis, and who were blinded to clinical assessment and fungal culture results. An Esaote My Lab 60© Ultrasound System (Esaote, Genova, Italy) with a transducer frequency range of 7–13 MHz, equipped with Doppler, was used. The most affected nail in each subject was selected to be scanned in grey-scale mode in order to detect morphological changes, and subsequently with power Doppler (PD) to detect abnormal blood flow.
Nails were scanned with the patient seated with the hand or foot in a standard position over the examination table, in a darkened room with a temperature between 22ºC and 25ºC. The probe was placed gently over the nail, with the transducer directed perpendicular to the surface and large amount of gel applied to the area examined in order to provide a correct acoustic interface.
The US routine included the assessment in grey-scale of quantitative parameters: thickness of the interplate space, ventral and dorsal nail plate contours, interplate space, longitudinal thickness of nail plate and bed (see below for definitions), matrix thickness and length, distal interphalangeal (DIP) periosteal surface, DIP space and contour, and distance between proximal nail plate and DIP. All measurements were repeated twice, and the mean value was used for the study. All the structures were assessed in longitudinal and transversal planes. In addition, the US qualitatively examined (echogenicity and lesions) the nail bed, plate and matrix, the extensor tendon and DIP.
Regarding the nail plate, 4 types of morphologic features were recorded according to Wortsman classification: focal hyperechoic deposits of the distal ventral plate (type I), loosening of the proximal ventral plate and normal dorsal plate (type II), appearance of wavy nail plates in both ventral and dorsal sections (type III) and loss of trilaminar structure of the ventral and dorsal nail plate sections (type IV) (15).
The thickness of the nail plate was defined as the distance between the dorsal and ventral plates, which appears in the US view as 2 hyperechoic lines with a hypoechoic space in between. The nail plate was assessed in longitudinal and transversal planes.
The nail bed was assessed in both longitudinal and transversal planes. Its thickness was defined as the distance between the ventral nail plate and the cortical surface of the DIP, which appears in the US view as the hypoechoic region under the nail plate.
The nail matrix is the echoic region at the proximal end of the nail plate; measurements were taken between this area and the cortical bone of the DIP in the longitudinal plane.
Extensor tendon US measurements included the tendon thickness at the level of the DIP joint and the PD signal within the tendon. To evaluate the PD signal, we used a 500–600 Hz pulse repetition frequency (PRF) with a dynamic range of 20–25 dB to increase the contrast between contiguous structures. Ultrasonographers were allowed to adjust the settings in order to produce the best quality images. The PD signal obtained was graded on the basis of the semi-quantitative validated scoring system from 0 to 3 (0: no signal PD; 1: confluent signal in < 25% of the nail bed area; 2: confluent signal in > 25% and < 50% of the nail bed area; and 3: PD signal in > 50% of the nail bed area) (16, 17).
Finally, the DIP joints were assessed in search of synovial fluid, synovial hypertrophy, joint PD signal, bone erosion and bone proliferation, according to OMERACT US group guidelines (18).
Prior to the study, the ultrasonographers reached a consensus on US acquisition, measurements and definitions of morpho-structural findings in the nail, based on existing literature. Test–re-test analysis was carried out for almost all relevant US findings from the first included 16 patients, in whom the images were evaluated a second time to assess inter-observer reliability. Intra-observer reliability was also measured in a second reading of the images.
Nail samples for fungal cultures were obtained by clipping the nail plate with a sterile nail clipper. Subungueal crumbling debris from underneath the nail plate was obtained for mycological culture in Sabouraud agar following standard procedures. Only those results that were positive for dermatophyte infection were included in the OM control group. In patients with negative fungal culture who were previously included due to a high clinical suspicion of fungal infection, a second sample was collected 1 month later from the same nail. If the second culture was also negative, these patients within the OM group were excluded from the study.
Means (standard deviation; SD) or counts and percentages were calculated for all continuous variables, and normality of sample distribution was assessed with the Shapiro–Wilk test. Both the test–retest reliability and inter-rater reliability of US were assessed with intra-class correlation coefficient (ICC2,2) with a 2-way mixed average measures model and absolute agreement. To interpret the results we adopted the classification by Brennan & Silman (19), in which ICC values > 0.8 indicate near-perfect agreement, 0.61–0.8 substantial agreement, 0.41–0.61 moderate agreement, 0.21–0.40 fair agreement, and < 0.2 poor agreement.
Comparisons between the US results of PsO and OM were tested using independent Student’s t-test for normally distributed data, or Mann-Whitney U test, as appropriate. To assess the ability of US to discriminate between OM and PsO, we estimated the area under the curve (AUC) of a ROC curve, with the diagnosis of the dermatologist as classification variable and nail bed power Doppler signal as test variable. Statistical analyses were performed using Stata version 14 (College Station, TX, USA). p-values less than 0.05 were considered statistically significant.
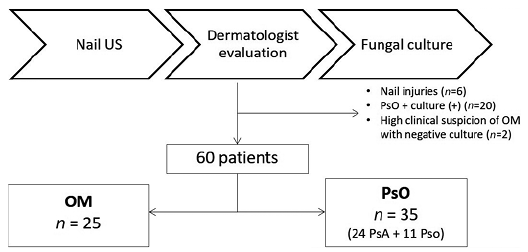
A total of 88 patients with nail involvement were eligible for the study. Six patients were excluded due to nail injuries that made the US difficult to interpret. Twenty patients (36%) with PsO and positive fungal culture were also excluded, as well as 2 patients with a high clinical suspicion of OM despite repeatedly negative cultures. A final total of 60 patients (35 with PsO and 25 with confirmed OM due to dermatophyte infection) were included in the study (Fig. 1) (60% women, mean age 50 years). OM was less frequent in hand nails (12%) than in toenails, while PsO occurred mainly in hand nails (57.2%; p < 0.001). The severity of nail alterations when applying NAPSI evaluation (for PsO and OM as well) was greater in OM (66%) than in PsO (35%) (Table I) although this did not reach statistical significance. The intra-reader ICC for the US measurements of nail plate and nail bed were good or very good (0.64–0.93), being less optimal for tendon thickness. The inter-reader ICC was 0.77 and 0.87 for nail plate, and 0.87 and 0.93 for nail bed (in transverse and longitudinal planes, respectively). These findings were again lower for assessment of tendon thickness (Table II). Nail bed and plate showed significantly less thickness in PsO compared with nails with OM (Table III). More than 80% of PsO and OM nails showed abnormalities on the nail plate. No significant differences were found according to nail plate disease based on Wortsman’s classification of PsO and OM, although the most prevalent type of nail plate disease was type II (28%) for PsO and type IV (32%) for OM (Table IV).
Fig. 1. Flow-chart of patients who met inclusion/exclusion criteria for the study population (n = 88).
Table I. Socio-demographic and Nail Psoriasis Severity Index (NAPSI) score from the included patients
Table II. Intra- and inter-rater test–re-test from a sample of patients (n = 16)
Table III. Quantitative ultrasound parameters of the studied nails. Comparison between psoriatic onychopathy and onychomycosis
Table IV. Morphological alterations detected by ultrasound in psoriatic onychopathy and onychomycosis patients
Patients with PsO had a significantly higher percentage of PD signal of nail bed graded 2 or higher than did patients with OM (60% vs. 16%; p < 0.006). The AUC to discriminate OM/PsO for nail bed PD signal was 0.706 (95% confidence interval (95% CI) 0.578–0.834) for a cut-off point of 3, sensitivity was 22.9%, and specificity was 96% (Table V), with a positive and negative likelihood ratio of 5.7 and 0.8, respectively (Fig. 2). In addition, nails with PsO showed significantly more frequent US structural damage in the DIP joint (erosions, irregularities or bone proliferation) than did nails with OM (62.8 vs. 8%; p < 0.001). There were no significant differences when comparing the presence of synovitis in PsO vs. OM (Table IV). For the rest of the clinically analysed variables no statistically significant differences were found between groups.
Fig. 2. Receiver operating characteristic (ROC) curve and area under the curve (AUC) for nail bed power Doppler signal 0.706, 95% confidence interval (95% CI) of AUC: 0.578–0.834, cut-off point ≥3, sensitivity=22.86%, specificity=96%, LR+ 5.7 LR– 0.8. LR: likelihood ratio.
Table V. Diagnostic utility analysis of the nail bed power-Doppler signal
To our knowledge, this is the first report comparing the US features of PsO and data for fungal infection. As a main finding, we observed significantly higher PD signal at the nail bed and US DIP alterations in patients with PsO compared with those with OM. The present study is relevant, since PsO may precede cutaneous or joint involvement in some patients and the morphological features of PsO are not exclusive to this disease. Furthermore, differential diagnosis from other conditions, especially OM, is a great challenge in clinical practice. During the last decade, research in the field of imaging in psoriatic arthritis has focused on the assessment of joints, entheses, or tendons, but little attention has been paid to finger and nail disease. Recently, imaging techniques, such as US, magnetic resonance image techniques or optical coherence tomography, have been applied to the study of psoriatic nails (17, 20–22).
In the current study, the difference between PsO and OM in terms of nail bed flow detected by US is the most relevant finding. Preliminary results demonstrated the potential role of PD signal in assessing the changes in blood flow in psoriatic plaque and PsO (8, 23, 24). Sandobal et al. (25), in agreement with our results, reported a high PD signal in the nailbed and DIP joints of patients with psoriatic arthritis. On the other hand, there are no studies assessing nail-bed blood-flow in patients with OM. Since OM is considered a disease with a very slow progression, the low PD signal we found was not unexpected.
The presence of arthritis in DIP joints, usually in the same finger that presents nail PsO, is a well-known psoriatic finding, and very plausibly corresponds to an extension of nail enthesopathy (10, 26–28). In this line, using US, we observed a significantly high percentage of patients with PsO who presented structural damage in the DIP compared with OM. Only 2 patients with OM presented structural damage, specifically bone proliferation. Both of these patients had hallux rigidus, and this bone proliferation was visible on radiographs. In contrast, we did not find more synovitis in PsO than in OM. In our study, only 22.9% of patients with PsO showed synovitis in the DIP joint on US, and 66% were in remission. The low activity we observed, together with a possible lack of sensitivity in detecting synovitis due to the US machines or probes used could explain this absence of a difference.
Some reports have described thickening of the extensor tendon insertion region, measured by US, in patients who presented PsO in the adjacent nail (27, 29, 30). In our study, however, we did not observe any significant differences between PsO and OM in the thickness or in the PD signal of the extensor tendon enthesis. This result may be explained by the low number of patients with PD signal in the extensor tendon described in our study, the type of probe used with low frequency (7–14 MHz), or the poor inter- and intra-observer reliability for tendon assessment.
In our study, the mean nail bed thickness for PsO was higher than the cut-off point established previously for unaffected nail bed (approximately 0.2 cm) (25, 29, 31). However, we found that fungal infection of the nail produces even greater nail-bed thickening than is observed in psoriasis. These results are in agreement with previous reports (15, 29, 31), although the differences we observed were not large despite their statistical significance, suggesting that this finding may not help substantially in distinguishing between both entities. The most frequent types of morphological change in the nail plate observed using Worstman typology (15) were type II in nail PSO and type IV in OM, similar to the changes observed by Sandobal et al. (25). In this sense, our data support the fact that nail fungal infection represents a more advanced stage of nail involvement than PsO. From a clinical point of view, patients with PsO more frequently presented hand involvement and notably less severe symptoms than did patients with OM according to NAPSI score. Although we cannot exclude a potential bias related to the inclusion of patients with PsO, the data observed are in accordance with previous reports (12).
This study is a cross-sectional study with a limited number of patients, despite being one of the largest studies published on this subject. The study mostly included cases of oil-drop lesions, so we cannot apply the data presented here to other PsO alterations. Although there is a wide clinical spectrum of nail disease related to PsO, oil-drop or salmon nail patches are not pathognomonic for PsO, but are quite frequent and represent the most controversial clinical sign in the differentiated diagnosis (32). In addition, histopathological examination would detect cases of OM with negative culture, and we selected only those cases with positive culture in the OM group, and repeatedly negative in the PsO group in order to minimize cases of PsO with concomitant OM. Furthermore, the probe used for evaluation of superficial tissues was of low frequency, which is a recognized limitation in nail US studies, and the ultrasonographers could not be completely blinded to the skin psoriatic lesions in patients with severe disease despite being in a dark room. Finally, we did not include patients with PsO and concomitant OM, so our results cannot exclude this possibility. Studying a greater number of cases would allow patients to be grouped according to the severity of nail changes and the location of altered nails for a better comparison. These aspects are relevant when considering using US findings to distinguish differences in nail bed or nail plate morphology between OM and PsO in a limited number of cases.
In summary, this is the first study to explore the utility of US in differential diagnosis of PsO and OM. The results demonstrate a higher PD signal and a more frequent presence of structural damage in DIP joints in PsO (oil-drop patches) compared with OM. These findings may help in distinguishing PsO from OM. However, further studies using higher resolution US probes are necessary to validate these results.
The authors are indebted to Silvia Iniesta (Research Nurse, Department of Rheumatology, Hospital del Mar, Parc Salut Mar) for her outstanding help.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize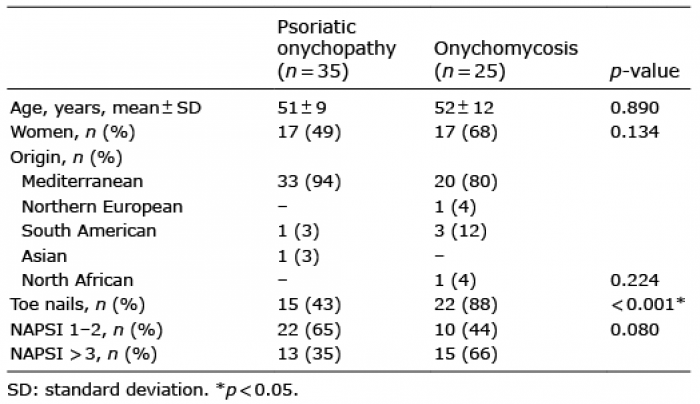 Click to show fullsize
Click to show fullsize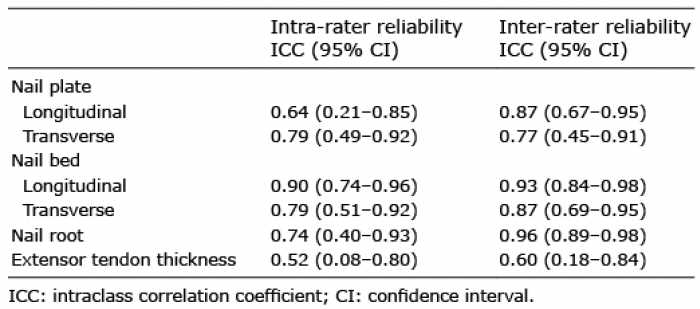 Click to show fullsize
Click to show fullsize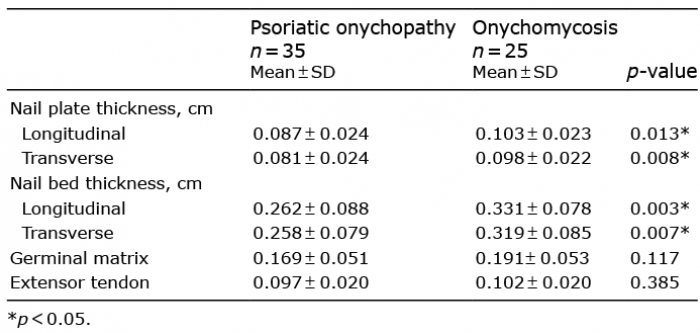 Click to show fullsize
Click to show fullsize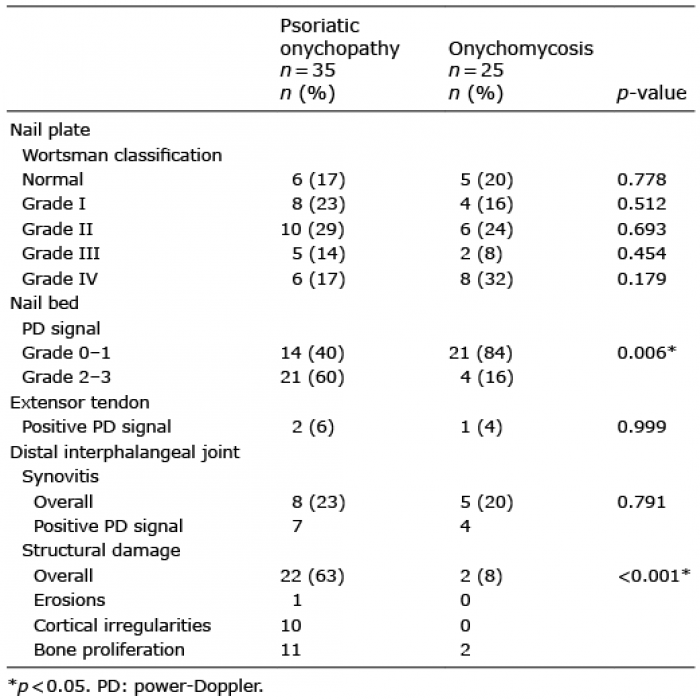 Click to show fullsize
Click to show fullsize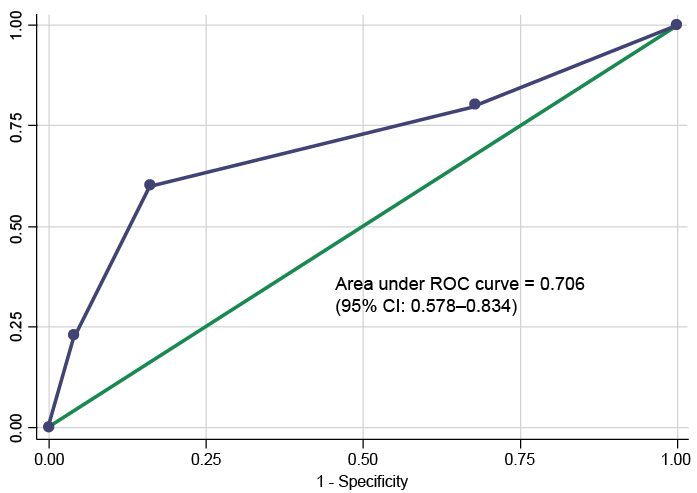 Click to show fullsize
Click to show fullsize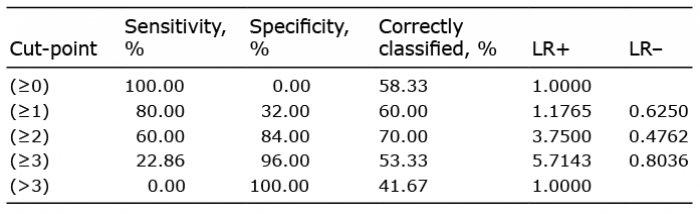 Click to show fullsize
Click to show fullsize