


1Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100730, PR China, and 2Department of Dermatology, Hospital Ramon y Cajal, Madrid, Spain. *E-mail: mdonglai@sohu.com
Accepted Oct 16, 2018; Epub ahead of print Oct 17, 2018
Porokeratosis is a heterogeneous group of skin disorders. Five clinical variants have been described: classic porokeratosis of Mibelli, disseminated superficial actinic porokeratosis, linear porokeratosis, punctate porokeratosis, and porokeratosis palmaris et plantaris disseminata. In 1995, Lucker et al. (1) described a subtype of porokeratosis: porokeratosis ptychotropica (PP). Clinically, this lesser-known entity most commonly affects body folds, especially the gluteal cleft, with or without involvement of the extremities. Male genitalia involvement is rare (2). We report here a special case of PP presenting with pruritic brownish verrucous plaques on the penis and scrotum.
A 48-year-old man presented with pruritic plaques on his penis and scrotum. The plaques had increased in size progressively over the last 20 years. Initial clinical presentation consisted of an itchy soybean-sized red scaly papule on the penis, but the lesions evolved to a verrucous scaly plaque, with a well-defined border accompanied by satellite lesion on the scrotum (Fig. 1). The patient reported having received topical treatment with 5-fluorouracil cream, with no resolution. He had no history of previous skin or general medical disorders. There was no family history of similar lesions. Routine haematological evaluations and serological tests for sexually transmitted diseases (HIV, hepatitis viruses, syphilis) were negative. A skin biopsy from the peripheral margin of the lesion on the penis revealed hyperkeratosis, acanthosis, and the presence of multiple cornoid lamellae. The dermis showed a mild lymphohistiocytic inflammatory infiltrate (Fig. 2). A diagnosis of porokeratosis ptychotropica was made. The patient was treated with pimecrolimus. After 3 months the lesions showed no improvement, but there was temporary relief of pruritus.
Fig. 1. Brownish, well-demarcated, hypertrophic, scaly, verrucous plaque on the penis and scrotum.
Fig. 2. Histopathology. (a) Hyperkeratosis, acanthosis, and the presence of multiple cornoid lamellae in the epidermis with a mild lymphohistiocytic inflammatory infiltrate in the dermis. (b) Multiple cornoid lamellae and disappearance of the granular layer underneath (haematoxylin and eosin (H&E), original magnification a: ×40, b ×100).
PP always presents as pruritic symmetrical red-brown verrucous papules and plaques with satellite areas of involvement. Histologically, PP is characterized by multiple cornoid lamellae, which may be related to the formation of hyperkeratotic plaques. In several cases, dermal amyloid deposits can be observed (3). Differential clinical diagnoses include lichen planus verrucosus, extramammary Paget’s disease, Bowen’s disease, and inflammatory linear verrucous epidermal nevus.
To date, the pathogenesis of PP remains unknown. Most cases occur sporadically and appear to be more frequent in male patients (4). Both genetic and environmental factors have been implicated, including ultraviolet light exposure, various infections, immunosuppression and repeated trauma (friction or scratching) (5).
Malignant transformation of porokeratosis occurs in 7.5% of cases (6). Long-term, extremity involvement, large-size lesions and ionizing radiation are the risk factors related to the malignant transformation of porokeratosis. Mazori et al. (7) reported a PP transforming into invasive squamous cell carcinoma for the first time. Therefore, periodic follow-up is recommended for the early diagnosis of potential squamous cell carcinomas, basal cell carcinomas, and melanomas.
PP appears to be refractory to conventional treatment. No standard treatment has been reported that shows complete clearance. Photodynamic therapy can be used as a therapeutic alternative treatment (8). Surgical approaches can be considered as an option for smaller lesions. A case of PP has been treated successfully with the dermatome (9). The patient was refractory to conventional treatments, and he was treated with a new approach using a dermatome to slice away the superficial tissue and showed complete remission (9).


 Click to show fullsize
Click to show fullsize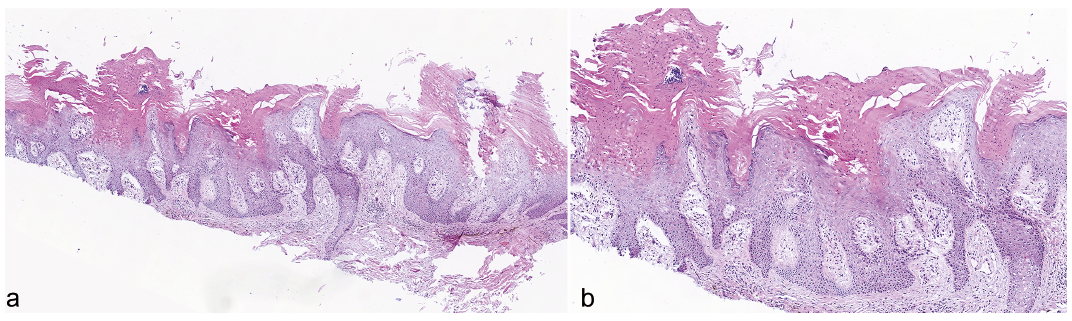 Click to show fullsize
Click to show fullsize