


Department of Dermatology and Allergy Centre, Odense University Hospital, DK-5000 Odense C, Denmark. E-mail: evy.paulsen@rsyd.dk
Accepted Nov 1, 2018; Epub ahead of print Nov 5, 2018
Classic pyoderma gangrenosum (PG) is an ulcerative skin disease that belongs to the neutrophilic dermatoses (1). Although the disease may be idiopathic, it has traditionally been associated with an array of conditions, notably inflammatory bowel disease and rheumatoid arthritis. The pathogenesis of PG is not fully clarified, but recent research suggests a pivotal role of pro-inflammatory cytokines, such as interleukin (IL)-1-β and IL-17 and tumour necrosis factor alpha (TNF-α), as in the monogenic autoinflammatory diseases (1). IL-1-β is also an atherogenic cytokine, and, in accordance with this, a recent clinical study showed evidence of more generalized inflammation in patients with PG: Jockenhöfer et al. (3) detected a stronger association between PG and the occurrence of metabolic syndrome than between PG and inflammatory bowel disease and rheumatic conditions (2, 3).
As might be expected from the pathogenesis, topical and/or systemic immunosuppressive or immunomodulating drugs are necessary for the healing of PG lesions. Despite this, the ulcers are sometimes quite recalcitrant to treatment.
A keratin-rich gel has been reported to be an effective topical treatment in ulcers and wounds of different origin (4–7). We report here our experience with this gel in a patient with PG ulcers.
A 62-year-old woman was referred to the department of dermatology with a suspected PG ulcer on her right shin in July 2014. Her past medical history was inconspicuous apart from arterial hypertension and recurrent ulcers. Since 2009, she had had 3 malleolar ulcers without evidence of venous, arterial, or coagulopathic aetiology. A skin biopsy from the third ulcer had been consistent with PG, and the patient was treated with topical and systemic corticosteroids, which resulted in rapid healing.
The present ulcer measured 3×4 cm on referral and despite treatment with systemic corticosteroids (prednisolone, up to 75 mg daily), supplemented first with cyclosporine 300 mg daily and later also with methotrexate 15 mg weekly, the ulcer progressed. Furthermore, a new ulcer developed symmetrically on the contralateral shin. Extensive blood tests and tumour positron emission tomography – computed tomography (PET-CT) scanning did not reveal any associated diseases. In December 2014, it was decided to discontinue cyclosporine and begin treatment with the TNF-α antagonist infliximab. After 3 infusions of infliximab, the ulcers measured 7×6 cm and 6×9.4 cm, respectively, and were covered with granulation tissue, but showed no sign of epithelialization (Fig. 1). Instead of diminishing the interval between the infliximab infusions, a keratin gel (Keragel®, Keraplast Technologies LLC, Christchurch, New Zealand) was applied to the ulcers as the main topical treatment in May 2015. At the next visit, after 9 days of treatment with the gel, the ulcers were diminished in size, and the systemic treatment with infliximab, corticosteroids, and methotrexate in tapering doses was continued along with Keragel® as topical treatment. In November 2015, the ulcers were healed (Figs 2 and 3). The infliximab infusions were not discontinued until October 2016 in order to prevent a relapse.
Fig. 1. Bilateral idiopathic pyoderma ulcers with granulation tissue in April 2015.
Fig. 2. Regressing pyoderma ulcers in July 2015 after 2 months’ treatment with keratin gel.
Fig. 3. Almost complete healing after 4 months’ treatment with keratin gel.
Although it is often necessary to use multiple anti-inflammatory drugs to treat PG ulcers, the drugs may have a negative effect on the final healing process. Thus, systemic corticosteroids impair wound healing both via global anti-inflammatory effects and on a cellular level by suppression of, for example, fibroblast proliferation and collagen synthesis, as well as through an increase in the risk of infection.
It is known that levels of TNF-α are elevated in chronic wounds, and that the concentration decreases during wound healing. Infliximab, both topically and systemically, may induce healing in ulcers of different origin, but a paradoxical development of PG in a patient treated with infliximab for psoriasis, has also been reported (8, 9). Thus, treatment with systemic immunosuppressive drugs is a double-edged sword; on the one hand impairing progression of the PG lesions, and on the other hand hindering the final steps in the healing of the lesions.
An important factor in the healing process is the func-tion of keratinocytes and keratin proteins (10). The first step in epithelialization is the migration of keratinocytes into the ulcer bed. An experimental study on keratin derived from ovine wool, showed that the oxidized keratin promoted keratinocyte migration and induced protein expression of type IV and type VII collagens, both of which are major components of the basement membrane (10). A clinical study on the use of dressings, containing wool-derived keratin, on refractory wounds of different origin supported the effect of keratin, with an overall response rate of 82% and a healing rate of 64% (4). Likewise, keratin products were shown to promote healing with minimal scarring in superficial and partial thickness burn injuries as well as being useful in the treatment of the lesions of patients with epidermolysis bullosa (6, 7, 11).
In the present case, the combination of infliximab, systemic corticosteroids, and methotrexate induced formation of granulation tissue, but the epithelialization lagged behind. Treatment with the keratin gel was chosen as an alternative to intensifying immune suppression and proved to be effective. According to some clinical reports, the resolution of pyoderma ulcers treated with infliximab may vary between 6 weeks and 24 months (12, 13). Although the effect of infliximab may not have reached its full potential, the healing seemed to accelerate after beginning the topical treatment with the keratin gel. Keragel® seems to be a safe and effective topical adjuvant in ulcers of immunological origin and especially useful to promote the last steps in the healing process. More controlled studies are needed to establish the usefulness of the keratin gel in the treatment of PG ulcers.
The authors thank Marie-Louise Little, Dianova A/S, for providing the gel for the patient.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize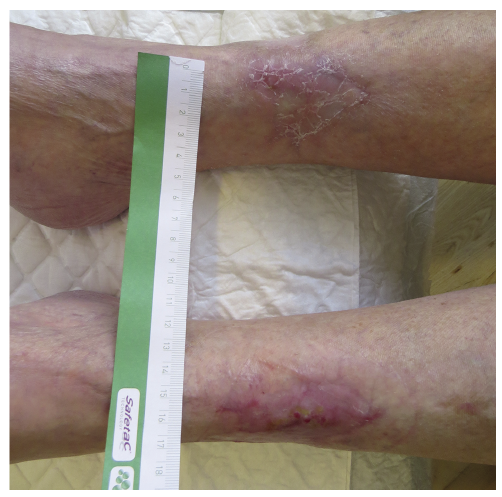 Click to show fullsize
Click to show fullsize