


¹PEDEGO Research Unit, University of Oulu, 2Department of Dermatology and Medical Research Center Oulu, and 3Department of Medicine, Oulu University Hospital, Aapistie 5A, FIN-90020 Oulu, Finland. E-mail: laura.huilaja@oulu.fi
Accepted Nov 14, 2018; Epub ahead of print Nov 14, 2018
Paraneoplastic acrokeratosis (Bazex syndrome) is a dermatosis associated with underlying malignancy, most often with squamous cell carcinoma of the upper aerodigestive tract (1). It typically occurs in middle-aged or older men with papulosquamous plaques over acral areas. During the course of the dermatosis skin symptoms spread over the trunk, extremities and scalp (1). Histological findings of paraneoplastic acrokeratosis are variable and the diagnosis is based on clinical findings (1, 2). In most cases cutaneous findings precede the malignant process for months or even a year (3, 4).
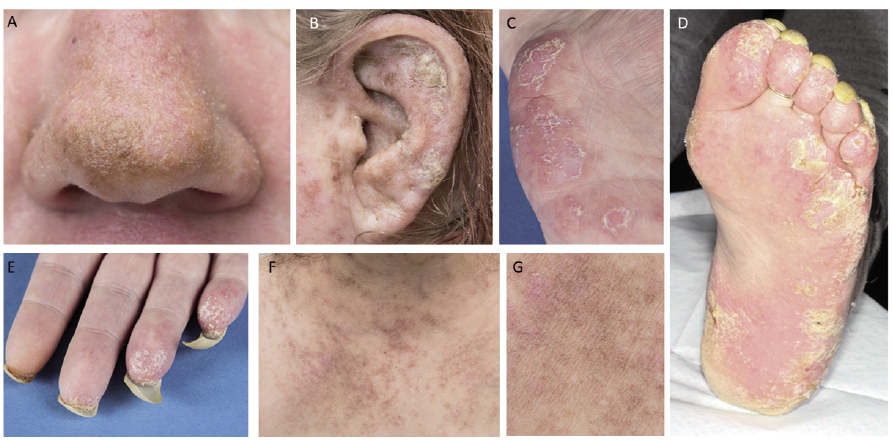
After obtaining informed consent, we report here the case of a 40-year-old healthy woman who was referred to the dermatologist with skin symptoms that had started 2 months earlier. At the time of consultation, she had a brownish hyperkeratosis on the helixes of the ears, tip of the nose and chin (Fig. 1a, b). The skin on the neck had spots of hyperpigmentation, but these were unpalpable. The hypothenar areas of the palms, fingertips (Fig. 1c, e) and soles had peeling psoriasis-like patches and she had a few urticarial lesions on the shins. There were follicularly highlighted reddish patches with some hyperkeratotic plaques on her chest and upper arms (Fig. 1f, g). Her hair was coarse and diffusely thinned. She had no other symptoms, but she reported having experienced pain in her fingers during recent months. Paraneoplastic acrokeratosis was considered and she was screened for the possible underlying malignancy by chest and breast radiography, abdomen ultrasound examination, gastroscopy, as well as examination by otorhinolaryngologist and gynaecologist with normal findings except mild unilateral pleuritis. Her blood cell count was normal except for slight thrombocytopaenia.
Fig. 1. Clinical presentation. Paraneoplastic acrokeratosis-like lesions as a skin finding of systemic lupus erythematosus (SLE). Brownish hyperkeratosis in (a) the nose tip and (b) the auricle. (c, d) Peeling, psoriasiformic patches in palms and soles. (e) Hyperkeratosis of the fingertips and under the nails. (f, g) Follicularly highlighted reddish patches on the chest.
After 2 months, the patient was febrile and had pain in her fingers and soles. Skin findings were even more prominent (Fig. 1d). Skin biopsy was ambiguous, with features of lichen sclerosus as well as scleroderma. Enlarged spleen and adenopathy in several areas was found in computer tomography (CT), followed by positron emission-CT (PET-CT) with similar findings and bilaterial pleural effusion. Lymphoma was suspected, but only reactive findings were seen in repeated lymph node biopsies. At this time, she had anaemia, thrombocytopaenia and leuco- and lymphopaenia. In addition, she had markedly elevated serum anti-nuclear antibody levels and hypocomplementaemia (Table I). Bone marrow specimen showed grade 1 myelofibrosis. Renal function was normal and she had no proteinuria. Based on these findings and her symptoms, she was diagnosed to have systemic lupus erythematosus (SLE). Direct immunofluorescence analysis of skin biopsy was also positive. Oral prednisolone (0.8 mg/kg) was initiated and within 2 weeks she was non-febrile, the cytopaenias started to recover and her skin symptoms gradually began to diminish.
Table I. Laboratory findings of the case described at the time of the diagnosis of systemic lupus erythematosus
This case demonstrates skin symptoms resembling paraneoplastic acrokeratosis in a patient with SLE. Despite extensive screening, no underlying malignancy was found. Skin symptoms are frequent in patients with SLE, but most often they are seen as malar rash or as similar findings as in cutaneous lupus erythematosus (5, 6). To best of our knowledge, paraneoplastic acrokeratosis-like symptoms has not been described previously as a skin manifestation of SLE. Of note, is that these symptoms can also associate with non-malignant conditions as we describe. However, it is highly important to intensively look for malignancy with repeated screenings (3) when managing a patient with paraneoplastic acrokeratosis-like symptoms.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize